营养摄取包括 Nutrient ingestion induces a substantial increase in mesenteric blood flow. In older persons (aged ≥ 65 years), particularly those with chronic medical conditions, the cardiovascular compensatory response may be inadequate to maintain systemic blood pressure during mesenteric blood pooling, leading to postprandial hypotension. In older ambulatory persons, postprandial hypotension is an important pathophysiological condition associated with an increased propensity for syncope, falls, coronary vascular events, stroke and death. In older critically ill patients, the administration of enteral nutrition acutely increases mesenteric blood flow, but whether this pathophysiological response is protective, or precipitates mesenteric ischaemia, is unknown. There are an increasing number of older patients surviving admission to intensive care units, who are likely to be at increased risk of postprandial hypotension, both during, and after, their stay in hospital. In this review, we describe the prevalence, impact and mechanisms of postprandial hypotension in older people and provide an overview of the impact of postprandial hypotension on feeding prescriptions in older critically ill patients. Finally, we provide evidence that postprandial hypotension is likely to be an unrecognised problem in older survivors of critical illness and discuss potential options for management.
Thu AN Nguyen, Yasmine Ali Abdelhamid, Liza K Phillips, Leeanne S Chapple, Michael Horowitz, Karen L Jones, Adam M Deane
Thu AN Nguyen, Yasmine Ali Abdelhamid, Leeanne S Chapple, Adam M Deane, Discipline of Acute Care Medicine, University of Adelaide, Adelaide 5005, Australia
Liza K Phillips, Michael Horowitz, Karen L Jones, Adam M Deane, National Health and Medical Research Council Centre for Research Excellence in Translating Nutritional Science to Good Health, Adelaide 5000, Australia
Liza K Phillips, Michael Horowitz, Endocrine and Metabolic Unit, Royal Adelaide Hospital, Adelaide 5000, Australia
Liza K Phillips, Michael Horowitz, Karen L Jones, Discipline of Medicine, University of Adelaide, Adelaide 5005, Australia
Adam M Deane, Intensive Care Unit, Royal Melbourne Hospital, University of Melbourne, Parkville, Victoria 3050, Australia
Author contributions: All authors equally contributed to this paper including conception and design of the study, literature review and analysis, drafting and critical revision and editing, and final approval of the final version.
Conflict-of-interest statement: No potential conflicts of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Adam M Deane, MBBS, PhD, Intensive Care Unit, Royal Melbourne Hospital, University of Melbourne, 300 Grattan Street, Parkville, Victoria 3050, Australia. adam.deane@adelaide.edu.au
Telephone: +61-3-93429234
Received: August 26, 2016
Peer-review started: August 27, 2016
First decision: December 13, 2016
Revised: December 16, 2016
Accepted: January 2, 2017
Article in press: January 3, 2017
Published online: February 4, 2017
Nutrient ingestion induces a substantial increase in mesenteric blood flow. In older persons (aged ≥ 65 years), particularly those with chronic medical conditions, the cardiovascular compensatory response may be inadequate to maintain systemic blood pressure during mesenteric blood pooling, leading to postprandial hypotension. In older ambulatory persons, postprandial hypotension is an important pathophysiological condition associated with an increased propensity for syncope, falls, coronary vascular events, stroke and death. In older critically ill patients, the administration of enteral nutrition acutely increases mesenteric blood flow, but whether this pathophysiological response is protective, or precipitates mesenteric ischaemia, is unknown. There are an increasing number of older patients surviving admission to intensive care units, who are likely to be at increased risk of postprandial hypotension, both during, and after, their stay in hospital. In this review, we describe the prevalence, impact and mechanisms of postprandial hypotension in older people and provide an overview of the impact of postprandial hypotension on feeding prescriptions in older critically ill patients. Finally, we provide evidence that postprandial hypotension is likely to be an unrecognised problem in older survivors of critical illness and discuss potential options for management.
Core tip: In older ambulatory persons, postprandial hypotension is an important pathophysiological condition associated with an increased propensity to coronary vascular events, stroke and death. In older critically ill patients, the administration of enteral nutrition acutely increases mesenteric blood flow, but whether this pathophysiological response is protective, or precipitates mesenteric ischaemia, is unknown. We herein describe the prevalence, impact and mechanisms and management of postprandial hypotension in older people. We finally provide an overview of the impact of postprandial hypotension on feeding prescriptions in and evidence that postprandial hypotension is likely to be an unrecognised problem in older survivors of critical illness.
Citation: Nguyen TA, Abdelhamid YA, Phillips LK, Chapple LS, Horowitz M, Jones KL, Deane AM. Nutrient stimulation of mesenteric blood flow - implications for older critically ill patients. World J Crit Care Med 2017; 6(1): 28-36
Ingestion of nutrients initiates a complex process involving precise coordination between the gastrointestinal tract, autonomic and cardiovascular systems to increase intestinal blood flow, whilst simultaneously maintaining circulatory homeostasis[1(opens new window),2(opens new window)]. Age and disease-related changes may compromise cardiovascular compensatory mechanisms, which, particularly in older persons, may result in a clinically relevant postprandial fall in blood pressure, known as postprandial hypotension (PPH). PPH is inconsistently defined but is generally regarded as a reduction in systolic blood pressure of ≥ 20 mmHg, or a decrease to ≤ 90 mmHg, that occurs within two hours of a meal and persists for at least 30 min[3(opens new window)]. This definition is empiric and derived from the definition of orthostatic hypotension[4(opens new window)]. It is important to recognise that although PPH frequently coexists with orthostatic hypotension, PPH is a distinct entity. However PPH may well occur more frequently, and have more substantive implications, than orthostatic hypotension[5(opens new window),6(opens new window)].
A recent meta-analysis reported that PPH occurs in about 20% of “healthy” older persons, about 30%-40% of nursing home residents, 20%-91% of hospitalised patients aged ≥ 65 years, about 40% of people with diabetes, and 40%-100% of patients with Parkinson’s disease[7(opens new window)]. The wide range of reported prevalence in each group reflect the small cohort sizes and the confounding effect of lack of standardisation of methodology between studies; including the definition of PPH, composition of test meal, timing of meal ingestion, technique and duration of blood pressure measurement, and use of concomitant medications. However, it is clear that in each of these groups the prevalence of PPH is high and that the very elderly and patients with diseases associated with autonomic dysfunction are at particular risk. Surprisingly, the prevalence of PPH in elderly survivors of critical illness has not been evaluated.
PPH is now recognised as an important pathophysiological condition, not only because of its high prevalence, but also due to the associated substantial morbidity and mortality[3(opens new window)]. In older people in the community, PPH is a strong predictor of syncope, falls, coronary events and stroke - irrespective of whether the individual has symptoms[8(opens new window)]. In a prospective study of 499 nursing home residents, Aronow et al[8(opens new window)] reported that the postprandial fall in systolic blood pressure was an independent risk factor for falls, coronary events, stroke and all-cause mortality. Supportive data are also provided by two case-control studies that report that the magnitude and prevalence of PPH are substantially greater in patients with a history of falls or syncope when compared to controls[9(opens new window),10(opens new window)]. Furthermore, in a five-year study of nursing home residents, PPH was found to be an independent determinant of mortality (RR = 1.79; 95%CI: 1.19-2.68); with a “dose-response”, such that all-cause mortality increased 13% for every 10 mmHg decrease in postprandial systolic blood pressure (RR = 1.13; 95%CI: 1.03-1.24)[11(opens new window)].
As indicated, preliminary data suggest that it is important to identify PPH even in those patients who are unaware of the condition. While PPH is associated with adverse outcomes, more than half (about 60%) of patients with PPH may be asymptomatic and, therefore, do not seek treatment[5(opens new window),6(opens new window)]. For example, Kohara et al[12(opens new window)] studied 70 patients hospitalised with essential hypertension and reported that the prevalence of lacunar infarcts was increased two-fold in patients with asymptomatic PPH. The strong association between “asymptomatic” PPH and stroke has also been evident in larger cohorts of older people residing in nursing home facilities and ambulatory older people living in the community[8(opens new window),13(opens new window)]. While this association does not establish causality, it provides a compelling rationale to diagnose PPH, which is a simple and inexpensive process[7(opens new window)], and to determine whether interventions that attenuate PPH mitigate the risk of adverse outcomes, such as cerebrovascular events[14(opens new window)]. The latter approach is to some extent compromised by the current lack of established effective management strategies[15(opens new window)].
# EFFECT OF NUTRIENT STIMULATION ON MESENTERIC BLOOD SUPPLY IN HEALTH
The presence of nutrients, particularly glucose and fats[16(opens new window)], in the small intestine stimulates secretion of several vasoactive gastrointestinal hormones that augment intestinal blood flow[17(opens new window)]. In response to direct contact with intraluminal nutrients, intestinal K-cells promptly secrete glucose-dependent insulinotropic peptide, and L-cells secrete glucagon-like peptide-1 and -2 (GLP-1 and GLP-2)[18(opens new window)] (Figure 1(opens new window)). There is a two-fold increase in blood flow through the superior mesenteric artery[3(opens new window),19(opens new window)], such that up to 20% of total blood volume is diverted to the gastrointestinal tract, which facilitates digestion and absorption of nutrients[17(opens new window)]. The magnitude of this increase in mesenteric blood flow is dependent on meal size and the rate of nutrient delivery from the stomach into the small intestine[20(opens new window),21(opens new window)]. In the research setting, the potential confounding effect of inter- and intra-individual differences in the rate of gastric emptying on PPH can be regulated by directly infusing nutrient into the small intestine[21(opens new window),22(opens new window)]. Utilising this technique, it is apparent that mesenteric blood flow increases when nutrient is delivered at a greater rate and, particularly, when carbohydrate or fat are ingested when compared to protein[16(opens new window),23(opens new window)].
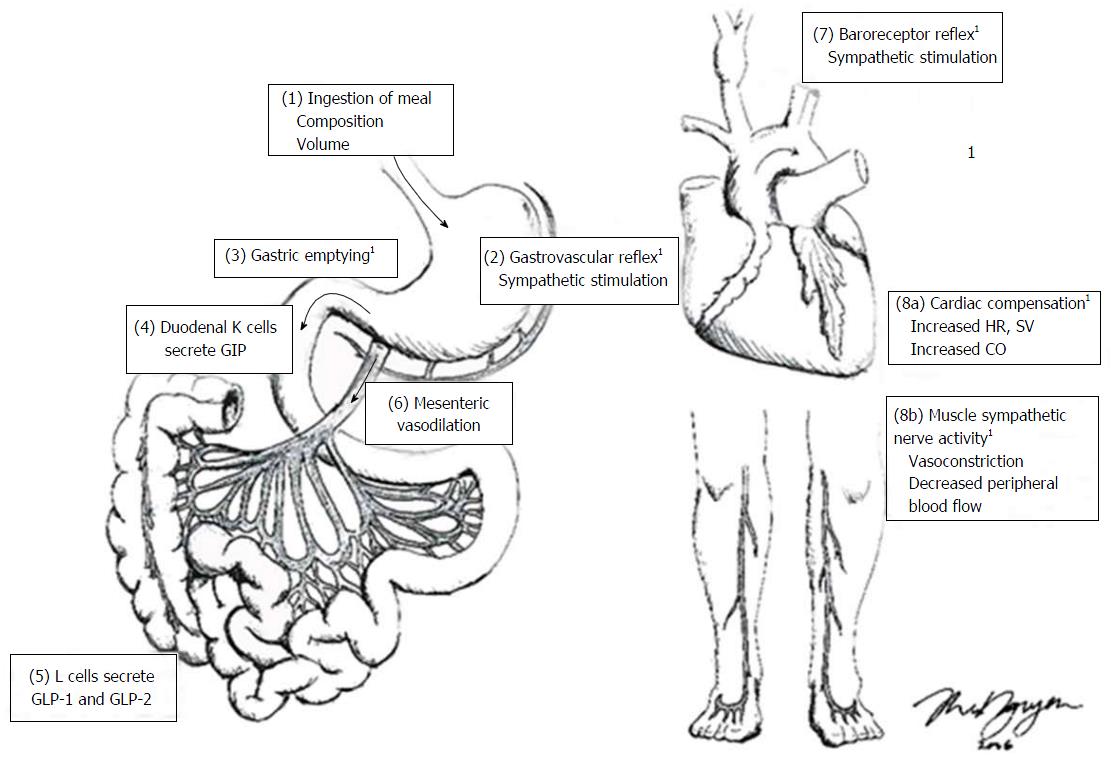
Figure 1 Factors involved in the regulation of postprandial blood pressure. (1) ingestion of a meal, with a greater carbohydrate load results in a greater postprandial hypotensive response; (2) Meal-induced gastric distension from the meal triggers stretch receptors in the stomach wall, increasing sympathetic nerve outflow; (3) gastric content is emptied into the small intestine, and, in response to the nutrient in the small intestine; (4, 5) gastrointestinal peptides are secreted from the small intestine (e.g., GLP-1 and GLP-2, glucagon-like peptide-1 and 2; GIP, glucose insulinotropic polypeptide); (6) gastrointestinal peptides stimulate mesenteric vessel dilation; (7) this results in reduced circulating blood volume and the reduction in blood pressure is detected by baroreceptors; (8a) the “gastrovascular” and baroreceptor reflexes stimulate sympathetic activity to increase heart rate (HR), stroke volume (SV) and thus cardiac output (CO) to maintain postprandial blood pressure; (8b) skeletal vasculature constricts to decrease peripheral blood flow. 1These factors are affected by age and have been identified as potential pathophysiological mechanisms of postprandial hypotension. Figure drawn by Ms. T. Nguyen. GIP: Glucose-dependent insulinotropic peptide; GLP: Glucagon-like peptide.
# PHYSIOLOGICAL HAEMODYNAMIC RESPONSES TO MEAL-INDUCED MESENTERIC BLOOD FLOW
In health, blood pressure is maintained even in the presence of postprandial mesenteric vasodilation via increases in cardiac contractility and peripheral vasoconstriction[3(opens new window)]. Meal-induced splanchnic blood pooling results in a temporary and virtual “hypovolaemia” that stimulates arterial baroreceptors[3(opens new window)], while gastric distension activates the “gastrovascular reflex”[24(opens new window)] (Figure 1(opens new window)). Together, these autonomic reflexes increase sympathetic nerve outflow to the heart and other vascular beds[5(opens new window),16(opens new window)] to increase both heart rate and stroke volume, thereby, augmenting cardiac output[3(opens new window)]. In parallel, the increase in muscle sympathetic nerve activity leads to a compensatory vasoconstriction of skeletal vasculature[25(opens new window)].
# MECHANISMS UNDERLYING POSTPRANDIAL HYPOTENSION IN AMBULANT OLDER PERSONS
The pathophysiology of PPH reflects multiple factors that impair reflex cardiovascular compensation[3(opens new window)]. Given that mesenteric blood flow appears to be essentially unaffected by age[22(opens new window)], it has been postulated that autonomic dysfunction is the main, albeit not sole contributor, to PPH[7(opens new window),26(opens new window),27(opens new window)]. Masuda et al[28(opens new window)]estimated that healthy older people require a two to three-fold increase in sympathetic nerve activity to maintain postprandial blood pressure. However, with age, the sensitivity of the gastrovascular and baroreceptor reflexes diminishes[25(opens new window),29(opens new window)], such that gastric distension may have minimal, or no effect, on plasma noradrenaline concentrations[3(opens new window)]. Consequently, the hypertensive and muscle sympathetic nerve activity responses following ingestion is blunted in apparently “healthy” older people[22(opens new window),25(opens new window)]. In addition, PPH is common in individuals with autonomic impairment associated with primary autonomic failure, multiple system atrophy, Parkinson’s disease or diabetes mellitus, conditions that are all prevalent in older people[30(opens new window)]. In autonomic failure, the postprandial increase in cardiac output is attenuated, indicative of a diminished compensatory response during mesenteric vasodilation[27(opens new window)].
# PHYSIOLOGICAL RESPONSES TO ENTERAL NUTRITION IN THE CRITICALLY ILL
Administration of enteral nutrition (EN) is part of standard care of critically ill patients, although the optimal timing for the commencement of EN in patients with shock, and/or who are receiving substantive doses of catecholamines, remains controversial[31(opens new window)]. EN has several theoretical advantages over parenteral nutrition, including the stimulation of mesenteric blood flow and bowel contractility, as well as the release of trophic hormones[31(opens new window)]. In addition, early (within 24-48 h) initiation of EN supports commensal bacteria and favours maintenance of the structural and functional integrity of the gut mucosal barrier, including the gut-associated lymphoid tissue[32(opens new window),33(opens new window)]. Consequently, feeding via the enteral route may limit bacterial overgrowth and attenuate translocation of gastrointestinal organisms and toxins[33(opens new window),34(opens new window)]. However, in patients with established shock, postprandial nutrient-stimulated demand for mesenteric blood flow may potentially complicate systemic haemodynamics, while the increase in mesenteric blood flow may be deleterious via reperfusion injury[35(opens new window)]. The clinical dilemma as to whether EN protects against, or exacerbates, mesenteric ischaemia during critical illness, has been reviewed by several groups[35(opens new window)-37(opens new window)].
# SLOWER GASTRIC EMPTYING IN CRITICALLY ILL PATIENTS MAY MITIGATE POSTPRANDIAL HYPOTENSION
Despite EN being a frequently administered intervention, there is a paucity of information regarding its effects on gastrointestinal peptides and mesenteric blood supply in the critically ill[38(opens new window),39(opens new window)]. However, because of the frequent delay in gastric emptying associated with critical illness[40(opens new window)], the rate of exposure of nutrient to the small intestinal mucosa is diminished in many patients[41(opens new window)] that should, intuitively, attenuate vasoactive gastrointestinal peptide secretion. Our group has, however, reported increases in fasting and postprandial GLP-1 concentrations in the critically ill, particularly in those with feed intolerance[42(opens new window)]. This may represent the effect of undigested carbohydrates and fats remaining in the distal small intestine and colon, resulting in sustained secretion of gastrointestinal peptides. Alternatively, this may be secondary to an increased sensitivity to hormone secretion or decreased hormone clearance during critical illness.
# IMPLICATIONS OF CHANGES IN MESENTERIC BLOOD SUPPLY DURING ENTERAL FEEDING
It has been suggested that administration of EN to those patients with haemodynamic compromise or hypoxia could be harmful[35(opens new window)]. According to this concept, fasting mesenteric blood supply is marginal, and the introduction of EN will increase demand beyond oxygen delivery capacity, thereby provoking mesenteric ischaemia[43(opens new window),44(opens new window)]. While non-occlusive mesenteric ischaemia occurs in < 1% of critically ill patients, it carries substantial mortality (up to 80% in some series)[45(opens new window)].
The pathophysiology of non-occlusive mesenteric ischaemia in the critically ill is incompletely understood, but it is usually preceded by hypotension or hypovolaemia[46(opens new window)]. It has been suggested that during systemic hypotension mesenteric blood supply may be “sacrificed” to preserve systemic blood pressure and, in the presence of artheromatous plaques, which are normally associated with subclinical stenosis, this leads to critical ischaemia[47(opens new window)]. It has also been proposed that disordered autoregulation of mesenteric vasculature causes intense vasospasm of the superior mesenteric artery, even when systemic blood pressure is normal, which may be exacerbated during reperfusion[48(opens new window)]. The tips of the intestinal villi are considered to be especially sensitive to ischaemia, particularly given their reliance on a so-called “counter-current exchanger system” for oxygen delivery[36(opens new window)]. Arterial blood is supplied viathe central arterial vessel that arborises at the tip of the villus forming a dense subepithelial network of capillaries and oxygen cross-diffuses from the central supplying vessel to the peripheral limb of the vascular hairpin loop[49(opens new window)]. It has been proposed that when mesenteric blood flow is compromised the velocity of blood flow in the hairpin vascular loops is decreased leading to extravascular oxygen shunting at the base of villi[49(opens new window)], which causes local oxygen deficits at the villi tips, ultimately resulting in ischaemic injury and cell death[36(opens new window),49(opens new window)].
The tips of intestinal villi are essential for nutrient absorption, and it has been hypothesised that non-specific symptoms of gastrointestinal intolerance represents one of the earliest signs of injury[46(opens new window)]. The presence of unabsorbed nutrient in the bowel lumen results in fluid shifts, bacterial overgrowth and fermentation, potentially causing marked bowel distension[46(opens new window)]. Patients may, therefore, initially present with nausea, diarrhoea, bloating and abdominal distension. According to this theory, as the bowel wall is stretched further, there is a progressive increase in capillary sludging and a reduction in mucosal perfusion[46(opens new window)]. The resultant increased mural and vascular permeability allows translocation of fluid, bacteria and toxins across the bowel wall, which induces third-space fluid shifts and activates a cascade of cytokines and oxidative radicals that exacerbate the ischaemic episode[48(opens new window)]. Furthermore, changes frequently associated with age, such as the presence of congestive heart failure, dysrhythmias or cardiogenic shock, are likely to exacerbate the processes in the development of mucosal ischaemia, thereby identifying older critically ill patients as a high-risk group[46(opens new window)]. However, previous case series of critically ill patients with non-occlusive mesenteric ischaemia include a large proportion of relatively young patients[50(opens new window),51(opens new window)], which appears inconsistent with the proposed events in this model of pathophysiology.
Moreover, there is conflicting data, which suggest that during a period of systemic hypotension EN is protective and may reduce, or even prevent, non-occlusive mesenteric ischaemia[43(opens new window)]. A number of studies in animal models have demonstrated that small intestinal nutrient stimulates superior mesenteric artery blood flow and mucosal microcirculatory flow[34(opens new window),43(opens new window),52(opens new window)-54(opens new window)]. However, it should be recognised that these studies frequently use relatively young animals and an “acute insult” model[55(opens new window)]. Therefore, extrapolation of these data to older critically ill humans, who characteristically have considerable co-morbid illnesses and have been receiving liquid EN for a number of days, should be made highly circumspectly.
There is also a concern that changes in mesenteric blood supply stimulated by EN will lead to redistribution of cardiac output to the mesenteric circulation, thereby, “stealing” blood/oxygen from other organs including the heart and brain[43(opens new window)]. It is well established that PPH is associated with coronary vascular events and stroke in the “healthy” ambulant older persons and hospitalised patients with hypertension potentially due to this “stealing” phenomenon[3(opens new window)]. Whether this phenomenon occurs in the critically ill, and has clinical implications, is unknown.
# NUTRIENT STIMULATES MESENTERIC BLOOD FLOW DURING CRITICAL ILLNESS
To improve understanding of mesenteric blood flow during enteral feeding in the critically ill several investigators have “bypassed” the stomach and delivered nutrient directly into the small intestine. Revelley et al[38(opens new window)] reported that a standard polymeric nutrient liquid administered via a postpyloric tube to nine patients one-day post-cardiopulmonary bypass, who were also receiving catecholamine support, was associated with an approximately 30% increase in postprandial hepatosplanchnic blood flow with minimal impact on systemic haemodynamics. Rokyta et al[56(opens new window)] also reported that standard polymeric nutrient liquid infused via a postpyloric tube to ten patients with severe sepsis (mean age 61 years and n = 8 receiving catecholamine support) increased hepatosplanchnic blood flow. These investigators found that blood pressure was unaffected by nutrient administration, but that there were modest increases in cardiac output, measured using pulmonary artery thermodilution, when EN was commenced[56(opens new window)]. However, both studies used indocyanine green clearance to measure hepatosplanchnic blood supply, which is dependent on adequate hepatic perfusion and function, and may well be less predictable in the critically ill than in health. Furthermore, both groups utilised a mixed nutrient liquid delivered at a rate (0.75 kcal/min), which is less than normal physiological gastric emptying (1-4 kcal/min)[21(opens new window)] and standard feeding regimens[57(opens new window),58(opens new window)]. Accordingly, this rate is not known to stimulate changes in mesenteric blood flow in ambulatory older people[22(opens new window)], and is not the rate of gastric emptying in many critically ill patients[59(opens new window)]. Our group evaluated the effect of liquid glucose (2 kcal/min) infused directly into the small intestine in critically ill patients aged ≥ 65 years[39(opens new window)]. Compared to healthy age-matched persons, we observed that postprandial mesenteric blood flow measured by duplex ultrasound is attenuated in older critically ill patients (n = 11, but only one patient had established shock and required exogenous noradrenaline), which was associated with reduced glucose absorption, while mean arterial pressure was unaffected by nutrient infusion at this rate[39(opens new window)].
In summary, while there are limited data relating to the acute effect of nutrient on mesenteric blood flow, it appears that nutrient does increase macrovascular blood flow. In older critically ill patients with shock, there is no clear evidence that EN precipitates or protects against mesenteric ischaemia, or exacerbates hypotension, in this group. Nonetheless, feeding prescriptions that limit delivery to ≤ 1.5 kcal/min of a mixed nutrient liquid are likely to be well tolerated.
# PREVALENCE AND OUTCOMES OF OLDER PEOPLE IN THE ICU
Given the aging population and improved survival to older age, there is an increasing demand for health care services in older persons, including services provided in the intensive care unit (ICU) for critically ill patients[60(opens new window),61(opens new window)]. Recent multicentre cohort studies indicate that > 50% of ICU admissions are for patients aged ≥ 65 years, with 8%-13% of admissions being the very old (aged ≥ 80 years)[60(opens new window),62(opens new window)]. Indeed, the prevalence of older critically ill patients admitted to ICUs is projected to rise by 3%-5% annually[60(opens new window),62(opens new window)]. The increased rate of hospitalisation and admission to ICU in this group is attributable, in part, to the higher prevalence of chronic illness and organ impairment associated with older age[63(opens new window)].
Mortality and health care resource utilisation during, and following, hospital stay in older ICU survivors are substantial[62(opens new window)]. Approximately 16% of ICU patients die in hospital, with older patients being two- to three-fold more likely to die, making up about 70% of ICU non-survivors[60(opens new window),62(opens new window)]. Six-months after hospital discharge, almost half of ICU survivors have presented to the emergency department and one-third required hospital readmission[62(opens new window)]. Within five years of hospital discharge, one-third of survivors of critical illness die, with about 70% of ICU non-survivors being aged ≥ 65 years[62(opens new window)]. Those who survive critical illness have a greater reduction in physical function post-ICU requiring more rehabilitation services and utilisation of long-term care facilities[62(opens new window),64(opens new window)]. Accordingly, it is evident that older survivors of ICU represent a group that may benefit from increased follow-up and novel interventions, particularly when considering the burden associated with health care utilisation following critical illness.
# POTENTIAL FOR PPH IN OLDER SURVIVORS OF CRITICAL ILLNESS
All critically ill patients, regardless of age, are at high risk of acute autonomic nerve dysfunction due to the insult critical illness inflicts on organs, which disrupts the inter-organ communication network[65(opens new window)]. Spectral analysis of heart rate variability is frequently used to assess sympathetic-parasympathetic balance and cardiorespiratory interactions non-invasively[65(opens new window)]. While the precise prevalence of autonomic dysfunction in the critically ill is unknown it appears to be is poor prognostic marker for patients within the ICU[65(opens new window)]. Acute autonomic dysfunction, as evidenced as attenuation in heart rate variability, has been reported to be associated with the development of multiple organ dysfunction, cardiac arrhythmias, and death, and it can persist for prolonged periods even after discharge from hospital[66(opens new window)-68(opens new window)]. Schmidt and colleagues prospectively followed 90 critically ill patients with score-defined multiple organ dysfunction (56 patients were on catecholamine support), and reported about 95% of patients had significantly reduced heart rate variability, which was not affected by the administration of sedatives or catecholamines[65(opens new window)]. These investigators also reported that heart rate variability was comparable in young (< 40 years, n = 9), middle aged (40-60 years, n = 31) and older (> 60 years, n= 45), but baroreflex sensitivity declined with age[65(opens new window)]. Given that the baroreceptor reflex and cardiac autonomic function are fundamental to the maintenance of postprandial blood pressure, it is intuitively plausible that older patients who survive critical illness and have autonomic dysfunction represent a group at risk of PPH. However, there is limited data as to the prevalence of PPH in survivors of critical illness and it is also possible that delayed gastric emptying or attenuated superior mesenteric blood flow, which are both observed during critical illness, persist after ICU, and this would mitigate the risk of PPH.
Management of PPH can be non-pharmacological, or pharmacological and attenuate PPH by targeting the mechanism(s) involved in the pathophysiology of PPH, as specified in Figure 1(opens new window)[15(opens new window)]. Interventions, such as consuming smaller, more frequent meals, reducing carbohydrate content and protein “pre-loads”, to reduce the rate of glucose absorption in the small intestine may be effective, as this has been postulated to reduce the magnitude and duration of increased mesenteric blood flow[23(opens new window)]. The simple task of drinking approximately 350 mL of water immediately prior to nutrient ingestion, to maximise gastric distension, attenuates PPH, probably via the gastrovascular reflex[69(opens new window)]. Gastric emptying can be slowed with the use of guar and other “pre-load” stimulants[15(opens new window)]. Inhibition of gastrointestinal peptides may also be achieved via the use of alpha-glucosidase inhibitors (e.g., acarbose) or somatostatin analogues (e.g., octreotide)[15(opens new window),70(opens new window)]. Alternatively, sympathetic nerve activity can be directly stimulated via postprandial exercise or caffeine[15(opens new window)]. However, the evidence to support the efficacy of these interventions is limited as studies have, for the main part been acute and limited to small cohorts, often including individuals who do not clearly meet the criteria for diagnosis of PPH. Nevertheless, the use of inexpensive interventions, such as eating smaller meals and drinking water may be sufficient to attenuate PPH.
PPH is recognised as an important pathophysiological condition, which is prevalent in older people (aged ≥ 65 years) living within the community, and is associated with considerable morbidity and mortality. Demographic changes have resulted in an older population within the ICU and this group is likely to be particularly susceptible to PPH due to their co-morbid conditions, as well as the frequent critical illness-associated autonomic dysfunction. While administration of EN will acutely increase mesenteric blood flow in this group, whether this pathophysiological response is protective, harmful, or has no effect on blood pressure, remains uncertain. Current management strategies for PPH are limited. Further work is required to determine the prevalence of this condition in older survivors of critical illness and evaluate novel interventions in this cohort.
Footnotes
Manuscript source: Invited manuscript
Specialty type: Critical care medicine
Country of origin: Australia
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): B
Grade C (Good): 0
Grade D (Fair): 0
Grade E (Poor): 0
P- Reviewer: Hortobagyi T S- Editor: Qi Y L- Editor: A E- Editor: Li D
Oberman AS, Gagnon MM, Kiely DK, Nelson JC, Lipsitz LA. Autonomic and neurohumoral control of postprandial blood pressure in healthy aging. J Gerontol A Biol Sci Med Sci. 2000;55:M477-M483. [PubMed(opens new window)]
2.
Takamori M, Hirayama M, Kobayashi R, Ito H, Mabuchi N, Nakamura T, Hori N, Koike Y, Sobue G. Altered venous capacitance as a cause of postprandial hypotension in multiple system atrophy.Clin Auton Res. 2007;17:20-25. [PubMed(opens new window)] [DOI(opens new window)]
3.
Jansen RW, Lipsitz LA. Postprandial hypotension: epidemiology, pathophysiology, and clinical management. Ann Intern Med. 1995;122:286-295. [PubMed(opens new window)]
4.
Freeman R, Wieling W, Axelrod FB, Benditt DG, Benarroch E, Biaggioni I, Cheshire WP, Chelimsky T, Cortelli P, Gibbons CH. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton Neurosci. 2011;161:46-48. [PubMed(opens new window)] [DOI(opens new window)]
5.
Imai C, Muratani H, Kimura Y, Kanzato N, Takishita S, Fukiyama K. Effects of meal ingestion and active standing on blood pressure in patients & gt; or = 60 years of age. Am J Cardiol. 1998;81:1310-1314. [PubMed(opens new window)]
6.
Maurer MS, Karmally W, Rivadeneira H, Parides MK, Bloomfield DM. Upright posture and postprandial hypotension in elderly persons. Ann Intern Med. 2000;133:533-536. [PubMed(opens new window)]
Aronow WS, Ahn C. Association of postprandial hypotension with incidence of falls, syncope, coronary events, stroke, and total mortality at 29-month follow-up in 499 older nursing home residents. J Am Geriatr Soc. 1997;45:1051-1053. [PubMed(opens new window)]
9.
Puisieux F, Bulckaen H, Fauchais AL, Drumez S, Salomez-Granier F, Dewailly P. Ambulatory blood pressure monitoring and postprandial hypotension in elderly persons with falls or syncopes. J Gerontol A Biol Sci Med Sci. 2000;55:M535-M540. [PubMed(opens new window)]
10.
Schoon Y, Olde Rikkert MG, Rongen S, Lagro J, Schalk B, Claassen JA. Head turning-induced hypotension in elderly people. PLoS One. 2013;8:e72837. [PubMed(opens new window)] [DOI(opens new window)]
11.
Fisher AA, Davis MW, Srikusalanukul W, Budge MM. Postprandial hypotension predicts all-cause mortality in older, low-level care residents. J Am Geriatr Soc. 2005;53:1313-1320. [PubMed(opens new window)] [DOI(opens new window)]
12.
Kohara K, Jiang Y, Igase M, Takata Y, Fukuoka T, Okura T, Kitami Y, Hiwada K. Postprandial hypotension is associated with asymptomatic cerebrovascular damage in essential hypertensive patients. Hypertension. 1999;33:565-568. [PubMed(opens new window)]
13.
Tabara Y, Okada Y, Uetani E, Nagai T, Igase M, Kido T, Ochi N, Ohara M, Takita R, Kohara K. Postprandial hypotension as a risk marker for asymptomatic lacunar infarction. J Hypertens. 2014;32:1084-1090; discussion 1090. [PubMed(opens new window)] [DOI(opens new window)]
14.
Parati G, Bilo G. Postprandial blood pressure fall: another dangerous face of blood pressure variability. J Hypertens. 2014;32:983-985. [PubMed(opens new window)] [DOI(opens new window)]
15.
Ong AC, Myint PK, Potter JF. Pharmacological treatment of postprandial reductions in blood pressure: a systematic review. J Am Geriatr Soc. 2014;62:649-661. [PubMed(opens new window)] [DOI(opens new window)]
16.
Gentilcore D, Hausken T, Meyer JH, Chapman IM, Horowitz M, Jones KL. Effects of intraduodenal glucose, fat, and protein on blood pressure, heart rate, and splanchnic blood flow in healthy older subjects. Am J Clin Nutr. 2008;87:156-161. [PubMed(opens new window)]
17.
Fara JW, Rubinstein EH, Sonnenschein RR. Intestinal hormones in mesenteric vasodilation after intraduodenal agents. Am J Physiol. 1972;223:1058-1067. [PubMed(opens new window)]
18.
Kar P, Cousins CE, Annink CE, Jones KL, Chapman MJ, Meier JJ, Nauck M, Horowitz M, Deane AM. Effects of glucose-dependent insulinotropic polypeptide on gastric emptying, glycaemia and insulinaemia during critical illness: a prospective, double blind, randomised, crossover study. Crit Care. 2015;19:20. [PubMed(opens new window)] [DOI(opens new window)]
19.
Kearney MT, Cowley AJ, Stubbs TA, Evans A, Macdonald IA. Depressor action of insulin on skeletal muscle vasculature: a novel mechanism for postprandial hypotension in the elderly. J Am Coll Cardiol. 1998;31:209-216. [PubMed(opens new window)]
20.
Puvi-Rajasingham S, Mathias CJ. Effect of meal size on post-prandial blood pressure and on postural hypotension in primary autonomic failure. Clin Auton Res. 1996;6:111-114. [PubMed(opens new window)]
21.
Vanis L, Gentilcore D, Rayner CK, Wishart JM, Horowitz M, Feinle-Bisset C, Jones KL. Effects of small intestinal glucose load on blood pressure, splanchnic blood flow, glycemia, and GLP-1 release in healthy older subjects. Am J Physiol Regul Integr Comp Physiol. 2011;300:R1524-R1531. [PubMed(opens new window)] [DOI(opens new window)]
22.
Trahair LG, Vanis L, Gentilcore D, Lange K, Rayner CK, Horowitz M, Jones KL. Effects of variations in duodenal glucose load on blood pressure, heart rate, superior mesenteric artery blood flow and plasma noradrenaline in healthy young and older subjects. Clin Sci (Lond). 2012;122:271-279. [PubMed(opens new window)] [DOI(opens new window)]
23.
O’Donovan D, Feinle C, Tonkin A, Horowitz M, Jones KL. Postprandial hypotension in response to duodenal glucose delivery in healthy older subjects. J Physiol. 2002;540:673-679. [PubMed(opens new window)]
24.
Vanis L, Gentilcore D, Hausken T, Pilichiewicz AN, Lange K, Rayner CK, Feinle-Bisset C, Meyer JH, Horowitz M, Jones KL. Effects of gastric distension on blood pressure and superior mesenteric artery blood flow responses to intraduodenal glucose in healthy older subjects. Am J Physiol Regul Integr Comp Physiol. 2010;299:R960-R967. [PubMed(opens new window)] [DOI(opens new window)]
25.
Fagius J, Ellerfelt K, Lithell H, Berne C. Increase in muscle nerve sympathetic activity after glucose intake is blunted in the elderly. Clin Auton Res. 1996;6:195-203. [PubMed(opens new window)]
26.
Lagro J, Meel-van den Abeelen A, de Jong DL, Schalk BW, Olde Rikkert MG, Claassen JA. Geriatric hypotensive syndromes are not explained by cardiovascular autonomic dysfunction alone. J Gerontol A Biol Sci Med Sci. 2013;68:581-589. [PubMed(opens new window)] [DOI(opens new window)]
27.
Kooner JS, Raimbach S, Watson L, Bannister R, Peart S, Mathias CJ. Relationship between splanchnic vasodilation and postprandial hypotension in patients with primary autonomic failure. J Hypertens Suppl. 1989;7:S40-S41. [PubMed(opens new window)]
28.
Masuda Y, Kawamura A. Role of the autonomic nervous system in postprandial hypotension in elderly persons. J Cardiovasc Pharmacol. 2003;42 Suppl 1:S23-S26. [PubMed(opens new window)]
29.
van Orshoven NP, Oey PL, van Schelven LJ, Roelofs JM, Jansen PA, Akkermans LM. Effect of gastric distension on cardiovascular parameters: gastrovascular reflex is attenuated in the elderly.J Physiol. 2004;555:573-583. [PubMed(opens new window)] [DOI(opens new window)]
30.
Trahair LG, Kimber TE, Flabouris K, Horowitz M, Jones KL. Gastric emptying, postprandial blood pressure, glycaemia and splanchnic flow in Parkinson’s disease. World J Gastroenterol. 2016;22:4860-4867. [PubMed(opens new window)] [DOI(opens new window)]
31.
McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, McCarthy MS, Davanos E, Rice TW, Cresci GA. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016;40:159-211. [PubMed(opens new window)] [DOI(opens new window)]
32.
Jabbar A, Chang WK, Dryden GW, McClave SA. Gut immunology and the differential response to feeding and starvation. Nutr Clin Pract. 2003;18:461-482. [PubMed(opens new window)]
33.
Liew VY, Chapman MJ, Nguyen NQ, Cousins CE, Plummer MP, Chapple LA, Abdelhamid YA, Manton ND, Swalling A, Sutton-Smith P. A prospective observational study of the effect of critical illness on ultrastructural and microscopic morphology of duodenal mucosa. Crit Care Resusc. 2016;18:102-108. [PubMed(opens new window)]
34.
Gianotti L, Alexander JW, Gennari R, Pyles T, Babcock GF. Oral glutamine decreases bacterial translocation and improves survival in experimental gut-origin sepsis. JPEN J Parenter Enteral Nutr. 1995;19:69-74. [PubMed(opens new window)]
35.
McClave SA, Chang WK. Feeding the hypotensive patient: does enteral feeding precipitate or protect against ischemic bowel? Nutr Clin Pract. 2003;18:279-284. [PubMed(opens new window)]
Yang S, Wu X, Yu W, Li J. Early enteral nutrition in critically ill patients with hemodynamic instability: an evidence-based review and practical advice. Nutr Clin Pract. 2014;29:90-96. [PubMed(opens new window)] [DOI(opens new window)]
38.
Revelly JP, Tappy L, Berger MM, Gersbach P, Cayeux C, Chioléro R. Early metabolic and splanchnic responses to enteral nutrition in postoperative cardiac surgery patients with circulatory compromise. Intensive Care Med. 2001;27:540-547. [PubMed(opens new window)]
39.
Sim JA, Horowitz M, Summers MJ, Trahair LG, Goud RS, Zaknic AV, Hausken T, Fraser JD, Chapman MJ, Jones KL. Mesenteric blood flow, glucose absorption and blood pressure responses to small intestinal glucose in critically ill patients older than 65 years. Intensive Care Med. 2013;39:258-266. [PubMed(opens new window)] [DOI(opens new window)]
40.
Kar P, Jones KL, Horowitz M, Chapman MJ, Deane AM. Measurement of gastric emptying in the critically ill. Clin Nutr. 2015;34:557-564. [PubMed(opens new window)] [DOI(opens new window)]
41.
Deane AM, Rayner CK, Keeshan A, Cvijanovic N, Marino Z, Nguyen NQ, Chia B, Summers MJ, Sim JA, van Beek T. The effects of critical illness on intestinal glucose sensing, transporters, and absorption. Crit Care Med. 2014;42:57-65. [PubMed(opens new window)] [DOI(opens new window)]
42.
Summers MJ, DI Bartolomeo AE, Zaknic AV, Chapman MJ, Nguyen NQ, Zacharakis B, Rayner CK, Horowitz M, Deane AM. Endogenous amylin and glucagon-like peptide-1 concentrations are not associated with gastric emptying in critical illness. Acta Anaesthesiol Scand. 2014;58:235-242. [PubMed(opens new window)] [DOI(opens new window)]
43.
Kazamias P, Kotzampassi K, Koufogiannis D, Eleftheriadis E. Influence of enteral nutrition-induced splanchnic hyperemia on the septic origin of splanchnic ischemia. World J Surg. 1998;22:6-11. [PubMed(opens new window)]
44.
Kles KA, Wallig MA, Tappenden KA. Luminal nutrients exacerbate intestinal hypoxia in the hypoperfused jejunum. JPEN J Parenter Enteral Nutr. 2001;25:246-253. [PubMed(opens new window)]
45.
Park WM, Gloviczki P, Cherry KJ, Hallett JW, Bower TC, Panneton JM, Schleck C, Ilstrup D, Harmsen WS, Noel AA. Contemporary management of acute mesenteric ischemia: Factors associated with survival. J Vasc Surg. 2002;35:445-452. [PubMed(opens new window)]
46.
Schunn CD, Daly JM. Small bowel necrosis associated with postoperative jejunal tube feeding. J Am Coll Surg. 1995;180:410-416. [PubMed(opens new window)]
47.
Fiddian-Green RG. Splanchnic ischaemia and multiple organ failure in the critically ill. Ann R Coll Surg Engl. 1988;70:128-134. [PubMed(opens new window)]
48.
Bradbury AW, Brittenden J, McBride K, Ruckley CV. Mesenteric ischaemia: a multidisciplinary approach. Br J Surg. 1995;82:1446-1459. [PubMed(opens new window)]
49.
Lundgren O, Haglund U. The pathophysiology of the intestinal countercurrent exchanger. Life Sci. 1978;23:1411-1422. [PubMed(opens new window)]
50.
Scaife CL, Saffle JR, Morris SE. Intestinal obstruction secondary to enteral feedings in burn trauma patients. J Trauma. 1999;47:859-863. [PubMed(opens new window)]
51.
Marvin RG, McKinley BA, McQuiggan M, Cocanour CS, Moore FA. Nonocclusive bowel necrosis occurring in critically ill trauma patients receiving enteral nutrition manifests no reliable clinical signs for early detection. Am J Surg. 2000;179:7-12. [PubMed(opens new window)]
52.
Inoue S, Lukes S, Alexander JW, Trocki O, Silberstein EB. Increased gut blood flow with early enteral feeding in burned guinea pigs. J Burn Care Rehabil. 1989;10:300-308. [PubMed(opens new window)]
53.
Gosche JR, Garrison RN, Harris PD, Cryer HG. Absorptive hyperemia restores intestinal blood flow during Escherichia coli sepsis in the rat. Arch Surg. 1990;125:1573-1576. [PubMed(opens new window)]
54.
Bortenschlager L, Roberts PR, Black KW, Zaloga GP. Enteral feeding minimizes liver injury during hemorrhagic shock. Shock. 1994;2:351-354. [PubMed(opens new window)]
55.
Bihari S, Maiden M, Deane A, Fuchs R, Fraser J, Bersten AD, Bellomo R. Preclinical research in critical care - the Australasian perspective. Crit Care Resusc. 2015;17:151-152. [PubMed(opens new window)]
56.
Rokyta R, Matejovic M, Krouzecky A, Senft V, Trefil L, Novak I. Post-pyloric enteral nutrition in septic patients: effects on hepato-splanchnic hemodynamics and energy status. Intensive Care Med. 2004;30:714-717. [PubMed(opens new window)]
57.
Alberda C, Gramlich L, Jones N, Jeejeebhoy K, Day AG, Dhaliwal R, Heyland DK. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med. 2009;35:1728-1737. [PubMed(opens new window)] [DOI(opens new window)]
58.
Peake SL, Davies AR, Deane AM, Lange K, Moran JL, O’Connor SN, Ridley EJ, Williams PJ, Chapman MJ. Use of a concentrated enteral nutrition solution to increase calorie delivery to critically ill patients: a randomized, double-blind, clinical trial. Am J Clin Nutr. 2014;100:616-625. [PubMed(opens new window)] [DOI(opens new window)]
59.
Kar P, Plummer MP, Chapman MJ, Cousins CE, Lange K, Horowitz M, Jones KL, Deane AM. Energy-Dense Formulae May Slow Gastric Emptying in the Critically Ill. JPEN J Parenter Enteral Nutr. 2016;40:1050-1056. [PubMed(opens new window)] [DOI(opens new window)]
60.
Bagshaw SM, Webb SA, Delaney A, George C, Pilcher D, Hart GK, Bellomo R. Very old patients admitted to intensive care in Australia and New Zealand: a multi-centre cohort analysis. Crit Care (London, England). 2009;13:R45. [PubMed(opens new window)] [DOI(opens new window)]
61.
Heyland DK, Stelfox HT, Garland A, Cook D, Dodek P, Kutsogiannis J, Jiang X, Turgeon AF, Day AG. Predicting Performance Status 1 Year After Critical Illness in Patients 80 Years or Older: Development of a Multivariable Clinical Prediction Model. Crit Care Med. 2016;44:1718-1726. [PubMed(opens new window)] [DOI(opens new window)]
62.
Hill AD, Fowler RA, Pinto R, Herridge MS, Cuthbertson BH, Scales DC. Long-term outcomes and healthcare utilization following critical illness--a population-based study. Crit Care. 2016;20:76. [PubMed(opens new window)] [DOI(opens new window)]
63.
Haas LE, Karakus A, Holman R, Cihangir S, Reidinga AC, de Keizer NF. Trends in hospital and intensive care admissions in the Netherlands attributable to the very elderly in an ageing population. Crit Care. 2015;19:353. [PubMed(opens new window)] [DOI(opens new window)]
64.
Campion EW, Mulley AG, Goldstein RL, Barnett GO, Thibault GE. Medical intensive care for the elderly. A study of current use, costs, and outcomes. JAMA. 1981;246:2052-2056. [PubMed(opens new window)]
65.
Schmidt H, Müller-Werdan U, Hoffmann T, Francis DP, Piepoli MF, Rauchhaus M, Prondzinsky R, Loppnow H, Buerke M, Hoyer D. Autonomic dysfunction predicts mortality in patients with multiple organ dysfunction syndrome of different age groups. Crit Care Med. 2005;33:1994-2002. [PubMed(opens new window)]
66.
Eick C, Rizas KD, Meyer-Zürn CS, Groga-Bada P, Hamm W, Kreth F, Overkamp D, Weyrich P, Gawaz M, Bauer A. Autonomic nervous system activity as risk predictor in the medical emergency department: a prospective cohort study. Crit Care Med. 2015;43:1079-1086. [PubMed(opens new window)] [DOI(opens new window)]
67.
Baguley IJ, Heriseanu RE, Felmingham KL, Cameron ID. Dysautonomia and heart rate variability following severe traumatic brain injury. Brain Inj. 2006;20:437-444. [PubMed(opens new window)] [DOI(opens new window)]
68.
Mazzeo AT, La Monaca E, Di Leo R, Vita G, Santamaria LB. Heart rate variability: a diagnostic and prognostic tool in anesthesia and intensive care. Acta Anaesthesiol Scand. 2011;55:797-811. [PubMed(opens new window)] [DOI(opens new window)]
69.
Deguchi K, Ikeda K, Sasaki I, Shimamura M, Urai Y, Tsukaguchi M, Touge T, Takeuchi H, Kuriyama S. Effects of daily water drinking on orthostatic and postprandial hypotension in patients with multiple system atrophy. J Neurol. 2007;254:735-740. [PubMed(opens new window)] [DOI(opens new window)]
70.
Jansen RW, Peeters TL, Lenders JW, van Lier HJ, v’t Laar A, Hoefnagels WH. Somatostatin analog octreotide (SMS 201-995) prevents the decrease in blood pressure after oral glucose loading in the elderly. J Clin Endocrinol Metab. 1989;68:752-756. [PubMed(opens new window)]

 Nutrient stimulation of mesenteric blood flow
Nutrient stimulation of mesenteric blood flow