自动调节的下限:是时候转变想法了?
The lower limit of autoregulation: time to revise our thinking?
Drummond JC. The lower limit of autoregulation: time to revise our thinking?. Anesthesiology. 1997;86(6):1431-1433. doi:10.1097/00000542-199706000-00034
DeepL 翻译 + 人工校对 To the Editor:-I am concerned that the popular conception regarding the normal lower limit of cerebral blood flow autoregulation (LLA), frequently identified as 50 mmHg, may be substantially in error. Clinically, one encounters frequent reference to the LLA in discussions regarding minimal acceptable blood pressures for patient management. [1] It has been argued that this relevance has been overemphasized (see below). [2] Nonetheless, the LLA is a widely quoted physiologic limit to which the anesthesia community, rightly or wrongly, has assigned considerable importance.
致编辑:关于脑血流自动调节的正常下限(LLA)这一流行概念,常认为是 50 mmHg ,可能问题很大,令人担忧。在临床上,人们在讨论病人管理的最低可接受血压时,经常会提到 LLA。[1] 有人认为,这种相关性被强调过头了(见下文)。[2] 然而,LLA 是一个被广泛引用的生理界限,无论对错,麻醉界对都其相当重视。
Depictions of autoregulation in many standard texts show an autoregulatory plateau between mean arterial pressures of 50 and 150 mmHg. It is likely that the common choice of a mean arterial pressure (MAP) of 50 mmHg as the LLA was significantly influenced by a figure in a review article by Lassen. [3] Lassen's depiction of an LLA of 50 mmHg was in turn an estimate based on data from an investigation by McCall (see Table 1) published in 1953. [4] That investigation was performed in pregnant volunteers at or near term, in whom blood pressure was lowered with hydralazine and veratrum viride. The former is a cerebral vasodilator, [5] and the effects of the latter on the cerebral circulation are undefined. Yet, despite of the meager database that identified 50 mmHg as the LLA for healthy humans, the definition has remained widely accepted without thorough confirmation. In part, this may be because the LLA for several animal species is also approximately 50 mmHg. Nonetheless, a review of the literature more recent than McCall's 1953 publication does not confirm that an LLA of 50 mmHg actually prevails in humans. The majority of data derived in healthy, normotensive, nonanesthetized adults argues that the LLA is not less than an average value of 70 mmHg. In addition, one investigation concluded that the threshold for symptoms of cerebral ischemia in some normotensive nonanesthetized subjects was a MAP of 55 mmHg, [6] i.e., above our accepted LLA threshold. Some of the available investigations, their methods, and the mean values for the lower limit of autoregulation are presented in Table 1.
许多标准行文中对自动调节这样描述,在平均动脉压 50 - 150 mmHg 之间有一个自动调节平台。平均动脉压(MAP)为 50 mmHg 作为 LLA 的普遍选择很可能是受到 Lassen 的一篇评论文章中一个数字的影响。[3] Lassen 对 50 mmHg 的描述又是根据 McCall 在 1953 年发表的调查数据(见表 1)而做出的估计。[4] 该调查是在怀孕或接近分娩的志愿者中进行的,用水蛭素和藜芦碱降低血压。前者是一种脑血管扩张剂,[5] 而后者对脑循环的影响尚不明确。然而,尽管将 50 mmHg 确定为健康人的 LLA 的数据集很小,但该定义仍被广泛接受,没有得到彻底的确认。在某种程度上,这可能是因为一些动物物种的 LLA 也大约是 50mmHg。尽管如此,对比 McCall 1953 年发表的文献的回顾并没有证实人类的 LLA 实际上是 50 mmHg。在健康的、血压正常的、非麻醉的成年人身上得到的大多数数据都认为,LLA 不低于 70mmHg 的平均值。此外,一项调查认为,在一些血压正常的非麻醉受试者中,脑缺血症状的阈值是 MAP 为 55mmHg,[6] 即高于我们接受的 LLA 阈值。表 1 中列出了一些现有的研究,列出了采用的方法以及自动调节下限的平均值。
Table 1. Data Regarding the Lower Limit of Autoregulation in Nonanesthetized, Normotensive Adults
表 1. 关于非麻醉、正常血压成人的自动调节下限的数据。
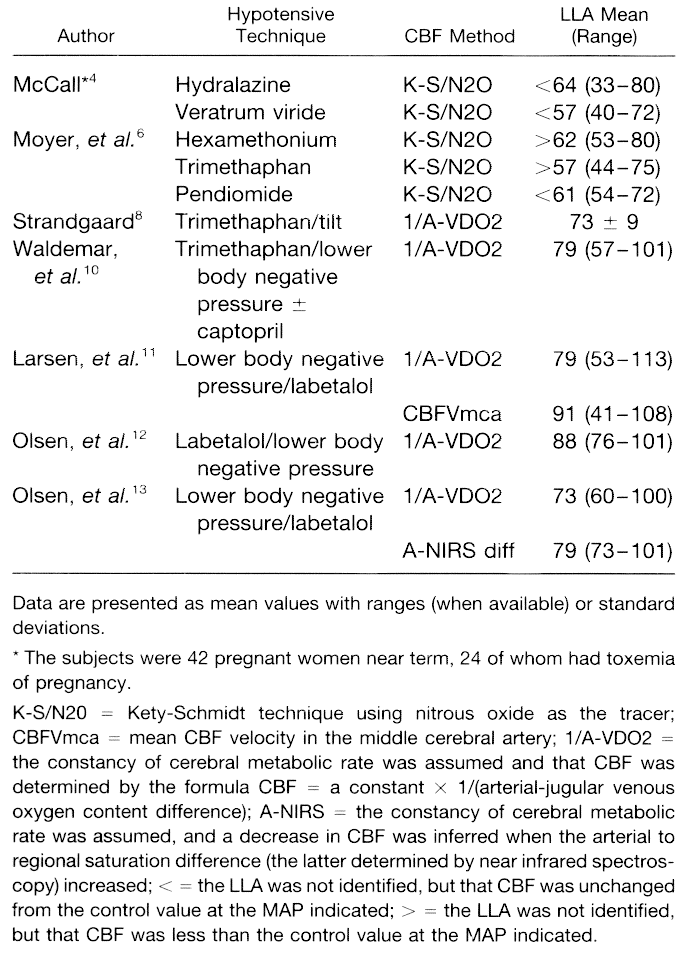
A review of the investigations in the table reveals other things about the LLA. The first is that the sharp inflection points of autoregulation curves are more a function of the statistical methods commonly used to calculate the LLA (linear regressions) than of normal physiology. These curves should probably be drawn with rounded “shoulders” rather than sharp “elbows.” But, more important, these investigations demonstrate that there is enormous individual-to-individual variation in the LLA (see ranges noted in Table 1)-so much so that a reviewer should wonder whether it can ever be appropriate to assume that any LLA value applies to a broad population of patients. If one insists on identifying an average value for a normotensive adult population to guide management, that average appears to be much higher than 50 mmHg.
对表中研究的回顾揭示了关于 LLA 的其他事情。首先是自动调节曲线的尖锐拐点,并非正常生理学功能如此,而是计算 LLA 常用的统计方法(线性回归)所致。这些曲线可能应该画成圆形的 "肩" 状,而不是尖锐的 "肘" 状。但是,更重要的是,这些调查表明,LLA 存在巨大的个体间差异(见表 1 中指出的范围)-- 那么,审查者应该怀疑,任何单一的 LLA 值用在广大的患者群体上是否合适?如果人们坚持要为血压正常的成年人群确定一个平均值来指导管理,那么这个平均值似乎要比 50 mmHg 高得多。
If one rejects the concept of an average LLA as providing useful clinical guidance, what is the alternative? Using resting MAP as the basis for an estimate of a patient's LLA (if and when relevant) rather than assuming that the patient will conform to a population average may be more appropriate. There are data that support this approach. The investigations of Finnerty, et al. and Strandgaard indicate that the LLA for individual nonanesthetized patients occurs at a MAP of approximately 25% less than the resting value and that symptoms of cerebral hypoperfusion appear when BP reaches 40–50% of the resting value. [[7,8] The ideal, of course, is for contemporary investigators to test the validity of this approach before it can be advocated with conviction.
如果人们拒绝将平均 LLA 值作为有用的指导临床的概念,那么有什么选择呢?使用静息 MAP 作为估计患者 LLA 的基础(如果有的话),而不是假设患者将符合人群的平均水平,可能更合适。有数据支持这种方法。Finnerty 等人和 Strandgaard 的调查表明,个别非麻醉病人的 LLA 发生在 MAP 比静息值低约 25% 的时候,当血压达到静息值的 40-50% 时,会出现脑灌注不足的症状。[7,8] 当然,最理想的是当代研究者在坚信不疑地倡导这种方法之前,先检验其有效性。
If the actual LLA in man is 70 mmHg or higher rather than 50 mmHg, so what? At a minimum, for the various authors (including me) who present, in standard textbooks, figures depicting the LLA in healthy subjects, it will mean either redrawing their diagrams or specifying the precise pharmacologic circumstances to which they apply. For those clinicians who define minimal acceptable MAPs in their patients on the basis of the normal LLA, it also will have relevance. Not all would accept the validity of such an approach in the first place because there should still be a considerable CBF reserve at this level [2] and because it has been amply demonstrated that many vasodilating agents, including anesthetic agents, lower the effective LLA. [2] It may eventually be argued that the widely published autoregulation curves accurately depict not “normal” autoregulation but rather “anesthetized” autoregulation for patients receiving certain anesthetics or vasoactive agents. In general, it appears that agents with a direct cerebral vasodilating properties lower the effective LLA. [2,9] However, there is certainly not sufficient dose-response information for the many anesthetic agents and combinations to permit the general conclusion that “anesthesia lowers the LLA.” One might anticipate little effect on the LLA by au courant total intravenous anesthesia regimens because the agents typically used lack cerebral vasodilating properties. The “bottom line” is that, if the LLA matters, it is unreasonable to assume that it is 50 mmHg for every normotensive adult in every anesthetic situation. The important clinical consequence is that in many patients, as MAP approaches 50 mmHg, we already may be well below the true LLA. Therefore, we may already be encroaching on the CBF reserve, and there may be a much smaller margin for error with respect to CNS ischemic injury than we have commonly believed.
如果人的实际 LLA 是 70 mmHg 或更高,而不是 50 mmHg ,那又如何?至少,对于那些在标准教科书中展示健康受试者 LLA 数字的作者(包括我)来说,这将意味着要么重新绘制他们的图表,要么明确他们所适用的确切药理情况。对于那些在正常 LLA 的基础上为病人定义最小可接受 MAP 的临床医生来说,这也会有意义。首先不是所有人都会接受这种方法的有效性,因为在这个水平上应该还有相当大的 CBF 储备 [2],而且已经充分证明,许多血管扩张剂,包括麻醉剂,会降低有效的 LLA。[2] 最终可以说,广泛发表的自动调节曲线准确描述的不是 "正常" 的自动调节,而是接受某些麻醉剂或血管活性药物的病人的 "麻醉" 自动调节。一般来说,具有直接脑血管扩张特性的药剂似乎会降低有效的 LLA。[2,9] 然而,对于许多麻醉剂和组合来说,肯定没有足够的剂量反应信息来得出 "麻醉会降低 LLA" 的一般结论。我们可以预计,目前的全静脉麻醉方案对 LLA 的影响很小,因为通常使用的药剂缺乏脑血管扩张的特性。底线 是,如果 LLA 很重要,那么假设每个正常血压的成年人在每种麻醉情况下都是 50 mmHg ,是不合理的。重要的临床结果是,在许多病人中,当 MAP 接近 50 mmHg 时,我们可能已经远远低于真正的 LLA。因此,我们可能已经启动了 CBF 储备,而且在中枢神经系统缺血性损伤方面的误差幅度可能比我们通常认为的要小得多。
The matter of the lower limit of autoregulation is more than a physiologic nicety. It is a concept that frequently influences clinical hemodynamic management. In that light, it may be appropriate for our community to adjust its thinking about the concept of the lower limit of cerebral autoregulation and, in particular, to escape the assumption that the lower limit of autoregulation is 50 mmHg in a majority of adults.
自动调节的下限问题不仅仅是一个生理学上的小问题。它是一个经常影响临床血流动力学管理的概念。有鉴于此,学界可能应该调整对脑自动调节下限概念的思考,特别是摆脱大多数成年人自动调节下限为 50 mmHg 的假设。
References
1.VanAken H, Miller ED: Deliberate hypotension, Anesthesia. Edited by Miller R. New York, Churchill Livingstone, 1994, pp 1491.
故意的低血压,麻醉。
2.McDowall DG: Cerebral blood flow and metabolism in acute controlled hypotension: implications for hypotensive anaesthesia. Acta Med Scand 1983; 678(Suppl):97-103.
急性控制性低血压的脑血流和代谢:对低血压麻醉的影响。
3.Lassen NA: Cerebral blood flow and oxygen consumption in man. Physiol Rev 1959; 39:183-238.
人的脑血流和耗氧量。
4.McCall ML: Cerebral circulation and metabolism in toxemia of pregnancy. Observations on the effects of Veratrum viride and apresoline (1-hydrazinophthalazine). Am J Obstet Gynecol 1953; 66:1015-30.
妊娠毒血症的脑循环和代谢:观察马鞭草和阿普里索林
5.Herpin D: The effects of antihypertensive drugs on the cerebral blood flow and its regulation. Prog Neurobiol 1990; 35:75-83.
抗高血压药物对脑血流的影响及其调节。
6.Moyer JH, Morris G, Smith C: Cerebral hemodynamics during controlled hypotension induced by the continuous infusion of ganglionic blocking agents (hexamethonium, Pendiomide and Arfonad). J Clin Invest 1954; 33:1081-8.
连续输注神经节阻断剂 (hexamethonium, Pendiomide and Arfonad) 引起的控制性低血压期间的脑血流动力学。
7.Finnerty FA, Wikin L, Fazekas JF: Cerebral hemodynamics during cerebral ischemia induced by acute hypotension. J Clin Invest 1954; 33:1227-32.
急性低血压引起的脑缺血期间的脑血流动力学。
8.Strandgaard S: Autoregulation of cerebral blood flow in hypertensive patients. Circulation 1976; 53:720-7.
高血压患者脑血流的自动调节。
9.Maekawa T, McDowall DG, Okuda Y: Brain-surface oxygen tension and cerebral cortical blood flow during hemorrhagic and drug-induced hypotension in the cat. Anesthesiology 1979; 51:313-20.
出血性和药物性低血压时猫的脑表面氧张力和大脑皮质血流量。
10.Waldemar G, Schmidt JF, Andersen AR, Vorstrup S, Ibsen H, Paulson OB: Angiotensin converting enzyme inhibition and cerebral blood flow autoregulation in normotensive and hypertensive man. J Hypertens 1989; 7:229-35.
血管紧张素转换酶的抑制和正常人和高血压人的脑血流自动调节。
11.Larsen FS, Olsen KS, Hansen BA, Paulson OB, Knudsen GM: Transcranial Doppler is valid for determination of the lower limit of cerebral blood flow autoregulation. Stroke 1994; 25:1985-8.
经颅多普勒对测定脑血流自动调节的下限有效。
12.Olsen KS, Svenden LB, Larsen FS, Paulson OB: Effect of labetalol on cerebral blood flow, oxygen metabolism and autoregulation in healthy humans. Br J Anaesth 1995; 75:51-4.
拉贝洛尔对健康人的脑血流、氧代谢和自动调节的影响。
13.Olsen KS, Svendsen LB, Larsen FS: Validation of transcranial near-infrared spectroscopy for evaluation of cerebral blood flow autoregulation. J Neurosurg Anesth 1996; 8:280-5.
经颅近红外光谱仪评估脑血流自动调节的验证。

 自动调节的下限
自动调节的下限