狗体外循环时常温和轻度低温的大脑压力-血流量的关系
狗体外循环时常温和轻度低温的大脑压力-血流量的关系
# 狗体外循环时常温和轻度低温的大脑压力 - 血流量的关系
Cerebral Pressure-Flow Relationship During Cardiopulmonary Bypass in the Dog at Normothermia and Moderate Hypothermia
Mutch WA, Sutton IR, Teskey JM, Cheang MS, Thomson IR. Cerebral pressure-flow relationship during cardiopulmonary bypass in the dog at normothermia and moderate hypothermia. J Cereb Blood Flow Metab. 1994;14(3):510-518. doi:10.1038/jcbfm.1994.63
DeepL 翻译 + 人工校对# 摘要
Summary: We studied cerebral autoregulation by analyzing cerebral pressure-flow curves during cardiopulmonary bypass (CPB) with alpha-stat (α-stat) acid-base management at 28 (n = 9) and 37°C (n = 9) in two groups of dogs. Cerebral blood flow (CBF) and cerebral metabolic rate for oxygen (CMRO2) were determined multiple times in each animal over an extensive range of cerebral perfusion pressure (CPP). The CPP was altered by changing perfusion flow rate. The dependence of CBF on CPP during normothermic and moderate hypothermic CPB was assessed using a block design analysis of covariance with CPP as the covariate. We anticipated maximal statistical power with this analysis to define if cerebral autoregulation was intact. This method of statistical analysis was compared with the conventional interpretation by linear regression analysis. Animals were administered sodium thiopental until an isoelectric electroencephalogram was obtained to assure stable depth of anesthesia independently of temperature effects. The animals were randomly assigned to either temperature group. The CBF was determined by injection of radioactive microspheres at each of five target CPPs randomly allocated (50, 60, 70, 80, and 90 mmHg). The brain oxygen content difference was defined as arterial minus superior sagittal sinus (SSS) oxygen content. No difference in CPP, hemoglobin, arterial carbon dioxide tension, or pH was seen between groups at any time period. In both groups, total CBF (tCBF) increased significantly with increasing CPP (p = 0.012 and 0.017 for normothermic and hypothermic CPB, respectively; CPP as covariate). The between-group difference in slopes (CPP × temperature effect) approached statistical significance (p = 0.059). For cerebral hemispheric CBF (hCBF), autoregulation was also impaired (p = 0.007 and 0.015, respectively). There was a significant between-group difference in slopes with a steeper slope for normothermia (p = 0.032). An inverse relation for arterial minus SSS oxygen content versus CPP was found (p = 0.0001 for both groups). The Q10 (the ratio of cerebral metabolic rates for oxygen for a 10°C change in temperature) was 3.8. In this study, using a block design analysis of covariance, tCBF was dependent on CPP during normothermia and moderate hypothermia with deep barbiturate anesthesia. We conclude that during CPB with α-stat acid-base management, the autoregulatory plateau was not horizontal for either temperature. In addition, for supratentorial structures (cerebral hemispheres), autoregulation was significantly more impaired for normothermia than for moderate hypothermia. Key Words: Cardiopulmonary bypass-Cerebral blood flowCerebral autoregulation-Dog.
摘要:我们通过分析两组狗在 28℃(n = 9)和 37℃(n = 9)的体外循环(CPB)和 alpha-stat(α-stat)酸碱管理期间的大脑压力 - 血流量曲线来研究脑部自动调节。在广泛的脑灌注压(CPP)范围内,多次测定每个动物的脑血流(CBF)和脑氧代谢率(CMRO2)。CPP 是通过改变灌注流速来改变的。在常温和中度低温 CPB 期间,CBF 对 CPP 的依赖性是用以 CPP 为协变量的区块设计协方差分析来评估的。我们预计这种分析具有最大的统计能力,以确定大脑自动调节是否完整。这种统计分析方法与线性回归分析的传统解释进行了比较。给动物注射硫喷妥钠,直到获得等电位脑电图,以确保麻醉深度稳定,不受温度影响。动物被随机分配到任一温度组。通过在随机分配的五个目标 CPP(50、60、70、80 和 90 mmHg )中的每一个注射放射性微球来确定 CBF。脑含氧量的差值被定义为动脉含氧量减去上矢状窦(SSS)含氧量。在任何时间段,组间的 CPP、血红蛋白、动脉二氧化碳分压或 pH 值都没有差异。在两组中,总 CBF(tCBF)随着 CPP 的增加而明显增加(常温和低温 CPB [体外循环] 分别为 p = 0.012 和 0.017;CPP 为协变量)。组间的斜率差异(CPP x 温度效应)接近统计学意义(p = 0.059)。对于大脑半球 CBF(hCBF),自动调节也受到损害(p = 0.007 和 0.015,分别)。组间的斜率有明显的差异,常温下的斜率更陡峭(p = 0.032)。发现动脉减去 SSS 氧含量与 CPP 呈反比关系(两组均为 p = 0.0001)。Q10(温度变化 10°C 时脑部氧气代谢率的比率)为 3.8。在这项研究中,使用块状设计的协方差分析,在常温和中度低温与深巴比妥酸盐麻醉期间,tCBF 取决于 CPP。我们的结论是,在 CPB [体外循环] 期间,在 α-stat 酸碱管理下,自动调节平台在两种温度下都不是水平的。此外,对于脑膜上结构(大脑半球)来说,常温下的自动调节功能明显比中度低温下的自动调节功能更差。
关键词:体外循环 - 脑血流 - 脑自动调节 - 狗。
# 序言
Cerebral blood flow (CBF) is felt to autoregulate over an extensive range of cerebral perfusion pressure (CPP). It is generally accepted that, at CPP from 50 to 130 mmHg, CBF is unchanged, that is, the autoregulatory plateau is horizontal. During cardiopulmonary bypass (CPB) with α-stat acid-base management (stable CO2 content irrespective of temperature; Swan, 1984), the cerebral circulation is also felt to autoregulate (Govier et aI., 1984; Murkin et aI., 1987; Aladj et aI., 1991). These studies indicate that CBF is independent of perfusion pressure over a range as great as 20-100 mmHg during moderate hypothermia. Other studies suggest that autoregulation may be impaired with deeper hypothermia, perhaps as a consequence of vasoparalysis (Greeley et aI., 1989; Taylor et aI., 1992). Thus, the influence of hypothermia on cerebral autoregulation during CPB is controversial. In contrast, little is known of cerebral autoregulation during normothermic CPB.
脑血流(CBF)被认为是在广泛的脑灌注压(CPP)范围内自动调节的。一般认为,在 CPP 为 50 至 130 mmHg 时,CBF 是不变的,也就是说,自动调节的平台是水平的。在体外循环 (CPB) 与 α-stat 酸碱管理 (无论温度如何,二氧化碳含量稳定;Swan, 1984) 期间,也感觉到脑循环的自动调节 (Govier et aI., 1984; Murkin et aI., 1987; Aladj et aI., 1991) 。这些研究表明,在中度低温期间,CBF 在 20-100 mmHg 的范围内是独立于灌注压的。其他研究表明,更深的低温可能会使自动调节功能受损,也许是血管麻痹的结果(Greeley 等人,1989 年;Taylor 等人,1992 年)。因此,低体温对 CPB 期间大脑自动调节的影响是有争议的。相比之下,人们对常温 CPB 期间的脑部自动调节知之甚少。
How cerebral autoregulation is determined during CPB may be open to interpretation as well. In most studies to date, data from measurements of CBF and perfusion pressure from multiple patients are usually pooled. Lack of a correlation between CBF and CPP by linear regression analysis is then taken to mean that autoregulation is preserved. Such an analysis assumes a linear cerebral pressure- flow relationship over the range of perfusion pressures examined among all patients, which may not be the case. The known influences on CBF such as temperature, hematocrit, arterial carbon dioxide tension (PaCO2) , anesthetic depth, and administration of vasodilators or vasopressors (Edvinsson et aI., 1993) are assumed to be controlled in an identical fashion for all subjects when CBF-CPP data are pooled. Control of all of these variables is quite difficult, especially in clinical studies. In addition, time-related decreases in CBF are not usually considered when analyzing pressure-flow curves with pooled data (Warach et aI., 1987; Rogers et aI., 1988; Prough et aI., 1991). Clearly, such timerelated effects can influence CBF and confound interpretation of the linear regression analysis of CBF-CPP data.
在 CPB 期间如何确定脑自动调节可能也是有待解释的。在迄今为止的大多数研究中,来自多个病人的 CBF 和灌注压的测量数据通常被汇集起来。通过线性回归分析,CBF 和 CPP 之间缺乏相关性,这就意味着自律调节被保留了。这样的分析假设在所有病人的灌注压范围内,大脑压力 - 血流量呈线性关系,但情况可能并非如此。对 CBF 的已知影响因素,如温度、血细胞比容、动脉二氧化碳分压(PaCO2)、麻醉深度以及血管扩张剂或血管抑制剂的使用(Edvinsson et aI., 1993),在汇集 CBF-CPP 数据时,假设所有受试者都以相同的方式进行控制。所有这些变量的控制是相当困难的,特别是在临床研究中。此外,在用集合数据分析压力 - 血流量曲线时,通常不考虑 CBF 中与时间有关的下降(Warach 等人,1987;Rogers 等人,1988;Prough 等人,1991)。显然,这种与时间相关的影响可以影响 CBF,并混淆 CBF-CPP 数据的线性回归分析的解释。
Thus, we hypothesized that (a) cerebral autoregulation might not be intact during α-stat CPB and (b) the experimental design and statistical analysis could influence the interpretation of whether autoregulation was intact. To address this issue, we have examined cerebral pressure-flow curves during CPB with α-stat acid-base management over a CPP range of 50-90 mmHg in each experiment, using a canine model. With this approach, CPP was altered in a random fashion by changing perfusion flow rate to control for time-related effects. Our experimental design allowed us to construct cerebral pressure-flow curves for each experiment. Such an approach permits a block design analysis of covariance (CPP as covariate). This approach increases statistical power by controlling for individual experimental effects, thereby decreasing the residual mean square error term (Steel and Torrie, 1960a). This statistical analysis was compared with the more common interpretation of cerebral autoregulation based on pooled pressure-flow data using linear regression analysis. We have examined the cerebral pressure-flow relationship at two clinically relevant temperatures for CPB (28 and 37°C).
因此,我们假设 (a) 在 α-stat CPB 期间,脑部自动调节可能不完整,(b) 实验设计和统计分析可能影响对自动调节是否完整的解释。为了解决这个问题,我们使用犬类模型,在每个实验中,在 50-90 mmHg 的 CPP 范围内,检查了 CPB 期间的大脑压力 - 血流量曲线。通过这种方法,CPP 以随机的方式被改变,通过改变灌注流速来控制与时间有关的影响。我们的实验设计允许我们为每个实验构建大脑压力 - 血流量曲线。这样的方法允许对协方差进行区块设计分析(CPP 为协变量)。这种方法通过控制单个实验效应来提高统计能力,从而减少残余均方误差项(Steel and Torrie, 1960a)。这种统计分析与更常见的基于集合压力 - 血流量数据的线性回归分析的脑自动调节解释进行了比较。我们研究了 CPB 的两个临床相关温度(28 和 37℃)下的大脑压力 - 血流量关系。
# 方法与材料
# 实验制备
Experimental preparation: The study was approved by the Committee for Animal Experimentation at the University of Manitoba. Eighteen mongrel dogs (22 ± 3 kg) were studied. All animals were anesthetized with sodium thiopental (25 mg/kg). The trachea was intubated and the animal ventilated with O2. The minute ventilation was adjusted to maintain PaCO2 at 35-40 mmHg. The dog was positioned in a stereotactic headframe in a modified sphinx position. Bipolar EEG electrodes were placed over the parietal hemisphere bilaterally and monitored by an Interspec Neurotrac in the raw EEG mode. Temperature was measured in the nasopharynx using a calibrated YSI telethermometer. Anesthesia was maintained with isoflurane 1.3% end-tidal [1 minimal alveolar concentration (MAC)] (Steffey and Howland, 1977) during the surgical preparation. Following thoracotomy, the isoflurane was discontinued for a minimum of 30 min and the EEG made isoelectric with a bolus of thiopental. A continuous infusion of thiopental was initiated at 10 mg kg - I h - I to maintain the EEG isoelectric during CPB. This was done to assure constant depth of anesthesia, independent of the effect that temperature has on volatile anesthetic agent partial pressures. Neuromuscular relaxation was achieved with pancuronium bromide.
实验制备: 本研究得到了马尼托巴大学动物实验委员会的批准。研究对象是 18 只杂种狗(22±3 公斤)。所有的动物都用硫喷妥钠(25mg/kg)进行麻醉。气管插管,用 O2 给动物通气。调整分钟通气量以保持 PaCO2 在 35-40mmHg。将狗安置在立体定向头架上,呈改良的斯芬克斯姿势。双极脑电图电极放置在双侧顶叶上,由 Interspec Neurotrac 以原始脑电图模式进行监测。使用校准的 YSI 电热计测量鼻咽部的温度。在手术准备期间,用 1.3% 的潮气量异氟烷 [1 个最小肺泡浓度(MAC)](Steffey 和 Howland,1977)维持麻醉。开胸手术后,停止使用异氟醚至少 30 分钟,用硫喷妥钠使脑电图呈等电状态。在 CPB 期间,开始连续输注硫喷妥钠,剂量为 10mg kg -1 h -1,以保持脑电图的等电性。这样做是为了确保恒定的麻醉深度,不受温度对挥发性麻醉剂部分压力的影响。用潘库溴铵实现神经肌肉松弛。
A flow-directed catheter was advanced through the left femoral vein into the right atrium for central venous pressure (CVP) monitoring. A femoral artery catheter was advanced into the distal aorta for mean arterial blood pressure (MABP) monitoring. A double-lumen (7.5 Fr) catheter was inserted into the left brachial artery for intermittent blood withdrawal. The superior sagittal sinus (SSS) was exposed by trephine and the posterior one third was cannulated nonocclusively by insertion of a 22- gauge intravenous catheter. Continuous cerebrospinal fluid pressure (CSFP) measurements were recorded by inserting a 22-gauge spinal needle into the cisterna magna with the use of a micromanipulator (Narishige). A right thoracotomy was performed. The right atrium and proximal aorta were cannulated with a single-stage 38 Fr atrial and J ostra 21 Fr or 24 Fr aortic cannula, respectively. Following the initiation of CPB, the left ventricle was vented by a cannula inserted through the right superior pulmonary vein, and the proximal aorta was occluded with a Seldinger vascular clamp.
一根导流导管通过左股静脉进入右心房进行中心静脉压(CVP)监测。一根股动脉导管被推进到远端主动脉以进行平均动脉血压(MABP)监测。一根双腔(7.5 Fr)导管插入左肱动脉进行间歇性抽血。通过环钻开孔暴露上矢状窦(SSS),并通过插入 22 号静脉导管对后三分之一置入非闭塞性空心管。通过使用显微操作设备(Narishige)将 22 号脊髓针插入脑脊液囊,记录连续脑脊液压力(CSFP)的测量结果。进行了右胸切开术。分别用单级 38 Fr 心房和 J ostra 21 Fr 或 24 Fr 主动脉插管插入右心房和近端主动脉。在启动 CPB 后,通过插入右肺上静脉的插管对左心室进行排气,用 Seldinger 血管钳对近端主动脉进行封堵。
All blood pressures and the CSFP were measured by calibrated Abbott transducers referenced to the intraauricular line. Data were recorded continuously on paper by an oscillograph (recorder model 7754A, Hewlett Packard) and intermittently on hard disk by an IBM PC-AT computer-based data acquisition system (Dataq Instruments). The latter data are reported. Arterial and SSS blood gases and hemoglobin were measured befor and after each microsphere injection by an ABL-3 Acid-Base Laboratory (Radiometer) at 37°C and not corrected for temperature.
所有的血压和 CSFP 都是由经过校准的 Abbott 传感器测量的,参考的是耳内线。数据由示波器(记录器型号 7754A,惠普公司)连续记录在纸上,并由基于 IBM PC-AT 计算机的数据采集系统(Dataq 仪器公司)间歇性地记录在硬盘上。后者的数据被报告。动脉血气和 SSS 血气以及血红蛋白是在每次注射微球之前和之后由 ABL-3 酸碱仪(Radiometer)在 37°C 测量的,没有经过温度校正。
Cardiopulmonary bypass was conducted utilizing a Travenol nonpulsatile roller pump with a Bentley 10 Plus bubble oxygenator and a Bentley arterial line filter (25 μm). The roller pump and oxygenator were primed with 2.5-3.0 L of lactated Ringer s and 1-2 units (500-1,000 ml) of canine whole blood in CPDA-I solution. The blood was obtained 48-72 h before the experiment from a donor animal and refrigerated at 4°C. The animal was systemically heparinized with 300-400 IU/kg of heparin (Organon: porcine intestine) and additional doses as required, to give an activated clotting time (ACT) ?400 s (Hemochron 400). Throughout the experiment, the animal had an intravenous infusion of lactated Ringer s at 200-250 ml/h containing NaHCO3• In Group N (normothermia), the intravenous solution contained 25 mEq/L of NaHCO3 and in Group H (hypothermia), it contained 12.5 mEq/L. This was done to maintain a stable hemoglobin concentration and acid-base state during the experiment (α-stat acid-base management). Norepinephrine (40 fLg) was injected into the oxygenator coincident with initiating CPB to minimize the hemodynamic consequences. The animals were randomized to one of two groups: Group N (n = 9; 37°C), Group H (n = 9; 28°C). Following the initiation of CPB, cooling or warming (if needed) commenced immediately in Groups H and N, respectively. Temperature was altered using a Travenol heat exchanger. In both groups of animals the mean CPP was maintained at 90 mmHg for 30 min to allow the animal to stabilize. Once the temperature was stable (no drift over 5 min), the CPP was randomly allocated to each of the following five target pressures: 50, 60, 70, 80, and 90 mmHg. The CPP was stabilized at the target pressure for a minimum of 10 min before flow determination.
体外循环是利用 Travenol 非脉冲式滚轴泵和 Bentley 10 Plus 气泡氧合器以及 Bentley 动脉管线过滤器(25 μm)进行的。滚筒泵和氧合器中加入了 2.5-3.0 升乳酸林格氏液和 1-2 个单位(500-1000 毫升)的 CPDA-I 溶液的犬全血。血液是在实验前 48-72 小时从献血动物那里获得的,并在 4℃下冷藏。用 300-400 IU/kg 的肝素(Organon:猪肠)对动物进行全身肝素化,并根据需要增加剂量,使激活凝血时间(ACT)达到 400 秒(Hemochron 400)。在整个实验过程中,动物以 200-250 毫升 / 小时的速度静脉注射含有 NaHCO3 的乳酸林格氏液 -- 在 N 组(常温),静脉注射液含有 25mEq/L 的 NaHCO3,在 H 组(低温),它含有 12.5mEq/L。这样做是为了在实验期间保持稳定的血红蛋白浓度和酸碱状态(α-stat 酸碱管理)。在启动 CPB 的同时,将去甲肾上腺素(40 fLg)注入氧合器,以尽量减少血液动力学后果。动物被随机分配到两组中的一组。N 组(n = 9;37℃),H 组(n = 9;28℃)。开始 CPB 后,H 组和 N 组分别立即开始降温或升温(如果需要)。使用 Travenol 热交换器来改变温度。两组动物的平均 CPP 维持在 90 mmHg 30 分钟,以使动物稳定下来。一旦温度稳定(5 分钟内没有漂移),CPP 被随机分配到以下五个目标压力中的每个。50、60、70、80 和 90mmHg。在测定流量之前,CPP 在目标压力下至少稳定 10 分钟。
# 脑血流的测量
Cerebral blood flow measurements: The radioactive microspheres, ultrasonicated in saline, were injected into the arterial cannula, -1 m proximal to the aortic root, after the PaCO2 was stable between 35-40 mmHg. If the PaCO2 could not be stabilized in this range by adjusting the O2 flow to the oxygenator, CO2 was added with a Sechrist mixer. Approximately 2.5 x 106 micro spheres ( 15 μm diameter) were injected into the arterial cannula. This number of microspheres assured >400 microspheres/sample for accurate blood flow measurement (Heymann et aI., 1977). The randomly selected microspheres were labeled with 46Sc, 85Sr, 141Ce (3M Company) or 95Nb, 113 Sn (New England Nuclear). A Harvard pump withdrew a reference blood sample for determination of organ blood flow (25 ml) from the brachial artery for 240 s, starting 15 s before injection of each microsphere.
脑血流的测量:在 PaCO2 稳定在 35-40 mmHg 之间后,将在生理盐水中超声处理过的放射性微球注入动脉插管,距离主动脉根部近端 1 米。如果通过调整氧合器的 O2 流量,PaCO2 不能稳定在这个范围内,则用 Sechrist 混合器加入二氧化碳。大约 2.5 x 106 个微球(直径 15 μm)被注入动脉插管。这一数量的微球保证了 > 400 个微球 / 样本,以实现精确的血流测量(Heymann et aI., 1977)。随机选择的微球被标记为 46Sc、85Sr、141Ce(3M 公司)或 95Nb、113Sn(新英格兰核公司)。Harvard 泵从肱动脉抽取用于测定器官血流的参考血样(25 毫升),持续 240 秒,在注射每个微球前 15 秒开始。
At the end of the experiment a lethal dose of thiopental was injected. The entire brain was excised. Following removal of the pia mater, the brain was sectioned into specific regions (left and right frontal, parietal, and occipital cortex, subcortical structures, cerebellum, and brainstem). The organ and blood samples were placed in a γ counter (LKB 1282 Compugamma) after being weighed. Counts/min were converted to regional blood flow (ml ml 100 g-1 min-1) with the use of standard equations (Hales, 1974).
在实验结束时,注射了致命剂量的硫喷妥钠。整个大脑被切除。在切除脊膜后,大脑被切成特定区域(左右额叶、顶叶和枕叶皮层、皮质下结构、小脑和脑干)。器官和血液样本经称重后被放入 γ 计数器(LKB 1282 Compugamma)。使用标准方程(Hales,1974)将计数 / 分钟转换为区域血流(ml 100 g-1 min-1)。
Total CBF (tCBF) in ml 100 g-1 min-1 was determined by summing weighted flows to all brain regions and dividing by total brain weight. Similarly, cerebral hemispheric CBF (hCBF) and brain stem CBF (bsCBF) were determined by the summation of weighted flows to the cerebral hemispheres and brain stem, respectively. The CPP was measured as (MABP - mean CSFP) and cerebral metabolic rate for O2 (CMRO2 ) as hCBF x (Art - SSS O2 content) in ml O2 100 g-1 min-1.
总 CBF (tCBF)(ml 100 g-1 min-1) 是由所有脑区的加权血流相加并除以总脑重而确定的。同样,大脑半球 CBF(hCBF)和脑干 CBF(bsCBF)分别由大脑半球和脑干的加权流量之和确定。CPP 为 (MABP - mean CSFP),大脑 O2 代谢率 (CMRO2) 为 hCBF x (Art - SSS 氧含量) ,单位是 ml O2 100 g-1 min-1。
# 统计分析
Statistical analyses: Changes over time for blood gas and hemodynamic variables were evaluated by analysis of variance (ANOV A) for repeated measures. When ANOV A was significant, comparisons were made with the leastsquares means test. Bonferroni s correction was applied (p < 0.05/n; where n = number of comparisons) when multiple comparisons were made. The corrected p value was considered statistically significant. The measurement scatter for regional CBF (rCBF) for the two groups was compared by Bartlett s test for homogeneity of variances (p < 0.05 considered significant). The cerebral pressureflow relationship for various brain regions was determined by block design analysis of covariance with CPP as the covariate. We looked for significant differences in slopes (CPP x experiment effect) and y intercepts (experiment effect) between the individual experiments (5 measurements relating rCBF to CPP in each experiment). If no differences in slopes or y intercepts were noted then the common slope and y intercept relating rCBF to CPP was used for further analysis. Between-group comparisons of slopes for the various brain regions was interpreted as the CPP x temperature effect from the statistical analysis; p < 0.05 was considered statistically significant. Block-design analysis of covariance was compared with the more usual linear regression analysis relating rCBF to CPP (globally pooling data from 45 separate observations (44 observations in Group N). The p values for the two statistical approaches were compared as an index of statistical power. A similar analysis was applied to the arterial - SSS oxygen content difference versus CPP data. Data are presented as mean ± SD.
统计分析:血气和血液动力学变量随时间的变化通过重复测量的方差分析(ANOV A)进行评估。当 ANOV A 有意义时,用最小二乘法平均数检验进行比较。当进行多重比较时,采用 Bonferroni 校正(p<0.05/n;其中 n = 比较的数量)。修正后的 P 值被认为具有统计学意义。两组区域 CBF(rCBF)的测量散点通过 Bartlett's 方差同质性测试进行比较(P < 0.05 被认为有意义)。各个脑区的脑压流关系是通过以 CPP 为协变量的区块设计协方差分析确定的。我们寻找各个实验之间的斜率(CPP x 实验效应)和 y 截距(实验效应)的显著差异(每个实验中有 5 个与 CPP 有关的 rCBF 测量)。如果没有注意到斜率或 y 截距的差异,则使用与 rCBF 和 CPP 相关的共同斜率和 y 截距进行进一步分析。各脑区斜率的组间比较被解释为统计分析中的 CPP x 温度效应;P < 0.05 被认为具有统计学意义。区块设计的协方差分析与更常见的 rCBF 与 CPP 相关的线性回归分析进行了比较(全球范围内汇集了 45 个独立观察点的数据(N 组有 44 个观察点)。两种统计方法的 P 值进行了比较,作为统计能力的指标。类似的分析被应用于动脉 - SSS 氧含量差异与 CPP 数据。数据以平均值 ±SD 表示。
# 结果
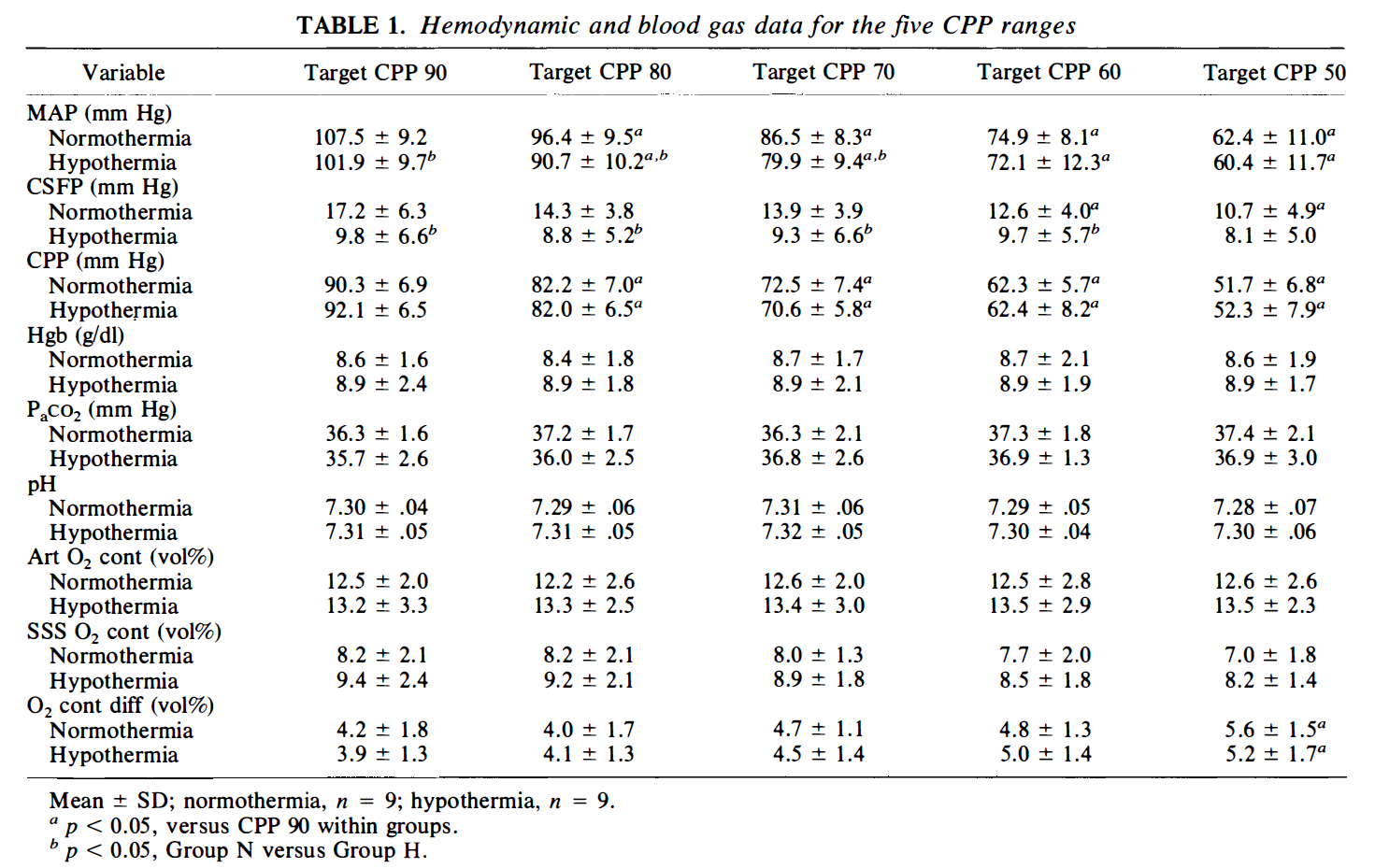
There were no significant differences between groups with respect to weight or to the dose of thiopental. For pooled data, the temperature in the normothermic group was 37. 0 ± 0.1°C and 27.6 ± 1. 0°C in the hypothermic group. Blood gas and hemodynamic data are shown in Table 1. The PaCO2, hemoglobin, and pH were well controlled within and between groups during all periods of injection of radioactive microspheres. Between groups there was a significantly greater MABP (p < 0. 05) during Flow I, 2, and 3 in Group N. This was associated with a significantly greater CSFP during these measurement periods, resulting in comparable CPP between groups for all five measurement periods.
各组之间在体重和硫喷妥钠的剂量方面没有明显的差异。就综合数据而言,常温组的温度为 37. 0 ± 0.1°C,低温组为 27.6 ± 1.0℃。血气和血液动力学数据显示在表 1 中。在注射放射性微球的各个时期,组内和组间的 PaCO2、血红蛋白和 pH 值都控制得很好。在组间,N 组的 MABP(P < 0. 05)在血流状态(通过血流控制 CPP 大小,共 5 种状态,b 标注的 p 值)1、2 和 3 期间明显较大,这与这些测量期间的 CSFP 明显较大有关,导致所有五个测量期间的组间 CPP 相当。
For the six brain regions examined (frontal, parietal, and occipital cortex, subcortical structures, cerebellum, and brain stem) there was no statistically significant difference in rCBF between the left and right sides, indicating adequate mixing of the radioactive microspheres.
对于所检查的六个脑区(额叶、顶叶和枕叶皮层、皮层下结构、小脑和脑干),左右两侧的 rCBF 没有统计学上的显著差异,表明放射性微球的充分混合。
The raw data for tCBF versus CPP for the two groups are shown in Fig. 1. There are 45 measurements in the hypothermic group and 44 in the normothermic group. One flow determination was discarded in the normothermic group because of faulty withdrawal of radioactive microspheres from the brachial artery. A noticeably greater scatter in tCBF is evident in the normothermic experiments. This impression was confirmed by comparing rCBF variances between the two temperature groups by Bartlett s test for homogeneity of variances. For all cases the variance of the rCBF data for Group N was significantly greater than that seen in Group H (p < 0.01 for all rCBF determinations).
两组的 tCBF 与 CPP 的原始数据显示在图 1。低温组有 45 次测量,常温组有 44 次。由于从肱动脉中提取放射性微球的操作失误,常温组的一个流量测定被放弃。在常温实验中,tCBF 的散射明显更大。通过 Bartlett's 变异性测试比较两个温度组之间的 rCBF 变异性,证实了这一印象。在所有情况下,N 组的 rCBF 数据的方差明显大于 H 组(所有 rCBF 测定的 p < 0.01)。
For both Group N and Group H, block design analysis of covariance indicated that there was no difference in individual slopes between experiments in each group [CPP x experiment effect (p = 0.4834 and 0. 1721 for Group N and Group H, respectively)] or individual y intercepts between experiments in each group [experiment effect (p = 0.8766 and 0.1810, respectively)]. The best-fit slope (CPP as covariate) was 0.43 ± 0.48 ml 100 g-1 min-1 mmHg-1 (p = 0.012) and y intercept 19 ± 39 for Group N. For Group H the best-fit slope was 0. 24 ± 0. 12 ml 100 g-1 min-1mmHg-1 (p = 0.017) and y intercept 0.65 ± 9.5. Because there were no significant CPP x experiment effects or experiment effects in either group, the covariate data for Group N could be reduced to an equation of the form tCBF = 0.43CPP + 19 (Fig. 1), whereas for Group H the covariate data were reduced to the equation tCBF = 0.24CPP + 0.65 (heavy dotted lines). Betweengroup difference in slopes approached statistical significance (p = 0.059).
对于 N 组和 H 组,区块设计协方差分析表明,每组实验之间的各个斜率 [CPP x 实验效应(N 组和 H 组分别为 p = 0.4834 和 0.1721)] 或每组实验之间的各个 y 截距 [实验效应(分别为 p = 0.8766 和 0.1810)] 没有区别。N 组的最佳拟合斜率(CPP 为协变量)为 0.43±0.48ml 100 g-1 min-1 mmHg-1(p = 0.012),y 截距为 19±39;H 组的最佳拟合斜率为 0.24±0.12ml 100 g-1 min-1 mmHg-1(p = 0.017),y 截距为 0.65±9.5。由于两组都没有明显的 CPP× 实验效应或实验效应,N 组的协变量数据可简化为 tCBF=0.43CPP+19 的方程式(图 1),而 H 组的协变量数据则简化为 tCBF=0.24CPP+0.65 的方程式(重虚线)。组间斜率的差异接近统计学意义(P = 0.059)。
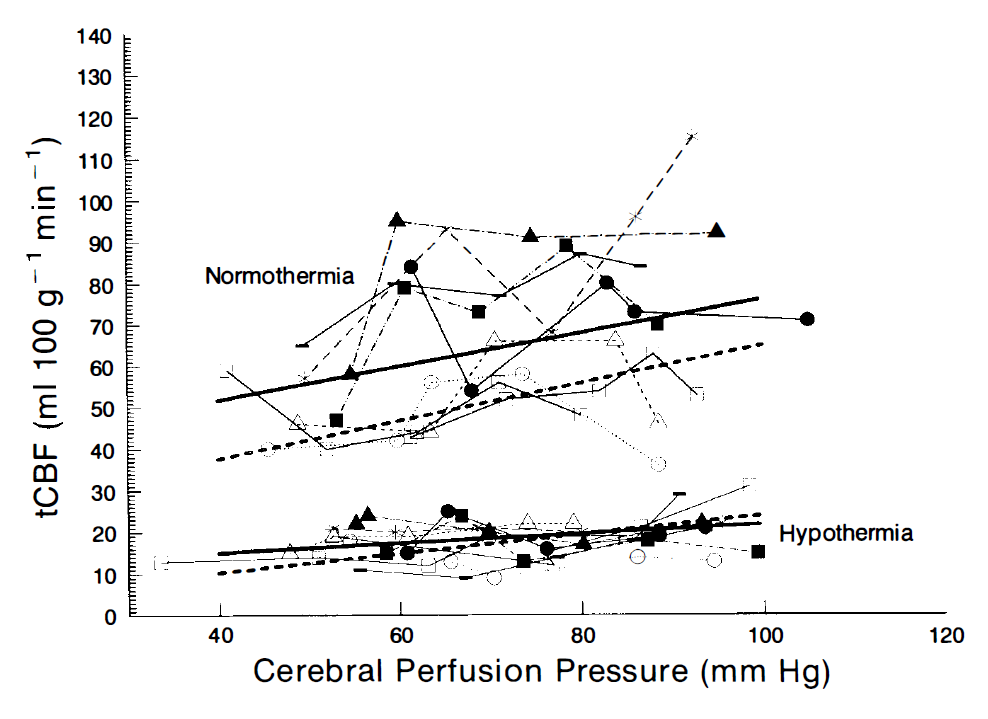
FIG.1.Raw data for tCBF versus CPP for both temperature groups.The slopes from block-design analysis of covariance are shown by the heavy dotted line in both temperature groups.The normothermic data were fit to the equation tCBF = 0.43CPP + 19 (p =0.012)and for the hypothermic data fit to the equation tCBF = 0.24CPP + 0.65 (p=0.017).Linear re- gression analysis for both groups is shown by the heavy solid line.The line of best fit for the normothermic data was tCBF = 0.43CPP + 35 (p 0.020) and for the hypothermic data was tCBF = 0.09cpp + 12 (p=0.049).
图 1 . 两个温度组的 tCBF 与 CPP 的原始数据。两个温度组的块设计协方差分析的斜率由重的虚线表示。常温数据被拟合为方程 tCBF = 0.43CPP + 19 (p =0.012),低体温数据拟合为方程 tCBF = 0.24CPP + 0.65 (p=0.017)。两组的线性再回归分析由粗实线显示。常温数据的最佳拟合线为 tCBF = 0.43CPP + 35 (p 0.020) ,低体温数据为 tCBF = 0.09cpp + 12 (p=0.049)。
For globally pooled data, a linear regression analysis of tCBF versus CPP is seen in Fig. 1. For Group N the heavy solid line is the solution to the least-squares regression analysis with tCBF = 0.43CPP + 35 (p = 0. 020). For Group H the heavy solid line is the solution to the equation tCBF = 0.09CPP + 12 (p = 0.049).
对于全部汇总数据,图 1 中看到了 tCBF 与 CPP 的线性回归分析。对于 N 组,粗实线是最小二乘回归分析的解决方案,tCBF=0.43CPP+35(p=0.020)。对于 H 组,粗实线是方程 tCBF = 0.09CPP + 12(p = 0.049)的解。
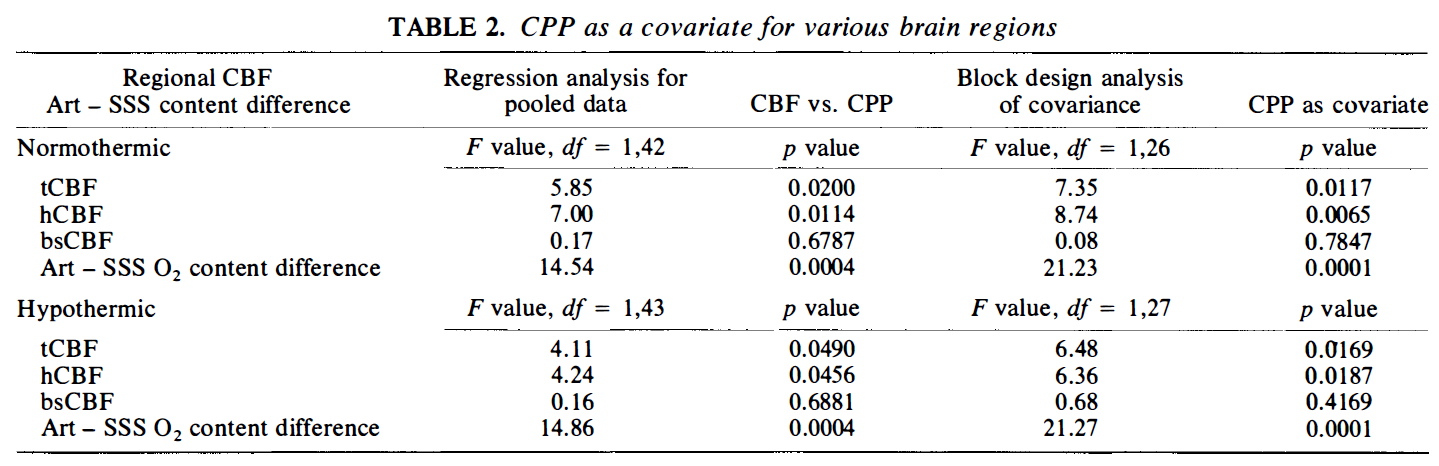
The block design analysis of covariance data and linear regression analysis data for hCBF and bsCBF versus CPP are shown in Table 2. In all instances the significance level (p value) associated with the block-design analysis of covariance was lower than that seen for linear regression analysis except for bsCBF with normothermia. However, for both groups brainstem structures did not have statistically significant slopes relating flow and pressure (Table 3). For hCBF, there was a significant between- group difference for slopes with a steeper slope present for normothermic data (p = 0.032). This was not the case for bsCBF (p = 0.999).
表 2 显示了 hCBF 和 bsCBF 与 CPP 的区块设计协方差分析数据和线性回归分析数据。在所有情况下,除常温下的 bsCBF 外,与区块设计协方差分析相关的显著水平(P 值)都低于线性回归分析的水平。然而,两组脑干结构都没有与流量和压力相关的统计学意义上的斜率(表 3)。对于 hCBF,常温数据的斜率有明显的组间差异,斜率较陡(P = 0.032)。而 bsCBF 则不是这种情况(p = 0.999)。
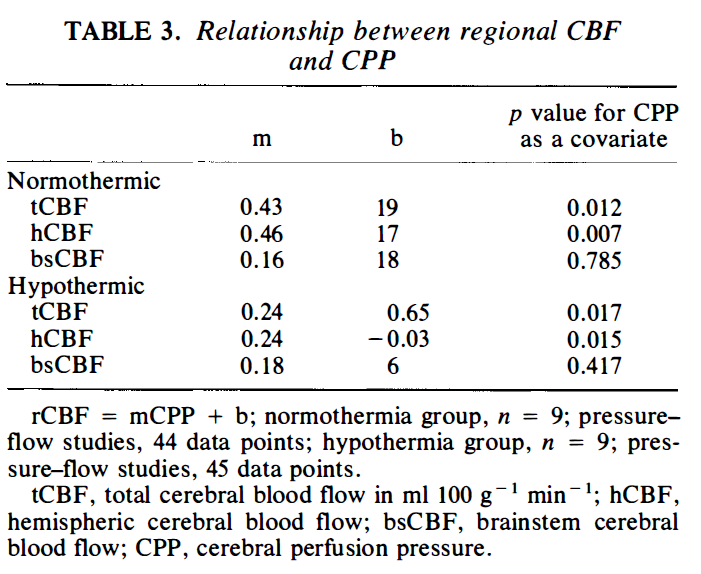
The inverse relationship between the arterial - SSS O2 contents versus CPP is shown in Fig. 2. For both groups, analysis of covariance revealed that CPP was a very strong covariate (p = 0.0001 for both). The arterial - SSS oxygen content differences across the cerebral hemispheres at given CPP values was very similar between the two groups.
动脉 - SSS O2 含量与 CPP 之间的反比关系见图 2。对于两组来说,协方差分析显示 CPP 是一个非常强的协变量(两者的 P=0.0001)。在给定的 CPP 值下,整个大脑半球的动脉 - SSS 氧含量差异在两组之间非常相似。
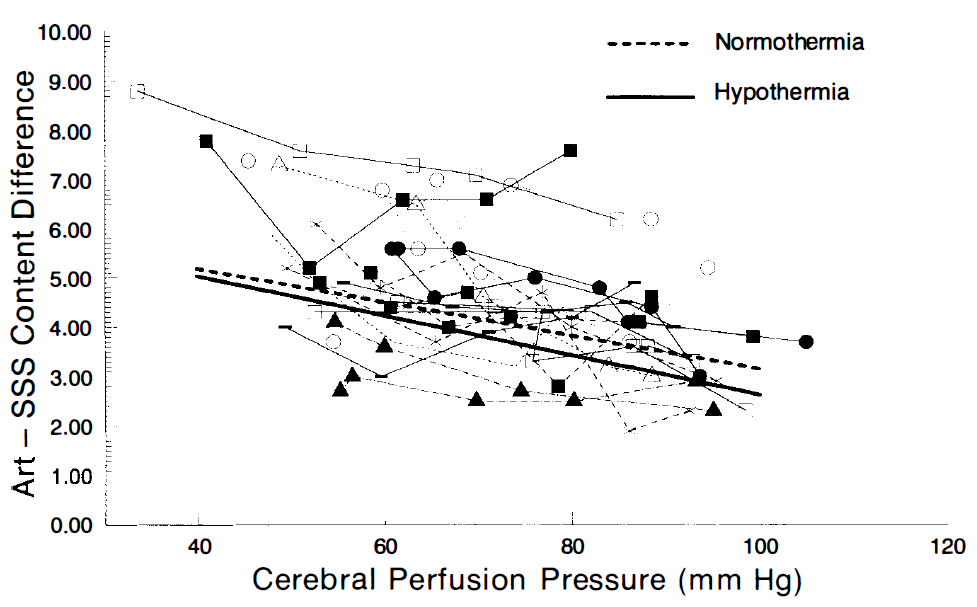
FIG. 2. Raw data for arterial - SSS oxygen content difference versus CPP for both temperature groups. The line of best fit for the normothermic group was Cont Diff = -0.037CPP + 7.0 (p = 0.0001) and for the hypothermic group Cont Diff = -0.039CPP + 6.6 (p = 0.0001).
图 2. 两个温度组的动脉 - SSS 氧含量差与 CPP 的原始数据。常温组的最佳拟合线为 Cont Diff = -0.037CPP + 7.0(p = 0.0001),低温组 Cont Diff = -0.039CPP + 6.6(p = 0.0001)。
In Group N, CMRO2 averaged 2. 8 ± 0.7 ml O2 100 g-1 min-1 and in Group H it was 0. 8 ± 0.2 ml O2 100 g-1 min-1 (p = 0.0001; between groups). The ratio of oxygen consumption over a 10°C temperature change (Q10) was 3.8 in this model. The CMRO2 versus CPP data are shown in Fig. 3. There was no correlation between these two variables in either group.
在 N 组,CMRO2 平均为 2.8±0.7 ml O2 100 g-1 min-1 ,在 H 组为 0.8±0.2 ml O2 100 g-1 min-1 (P = 0.0001;组间)。在这个模型中,10℃温度变化的耗氧量比率(Q10)为 3.8。CMRO2 与 CPP 的数据显示在图 3。两组的这两个变量之间没有相关性。
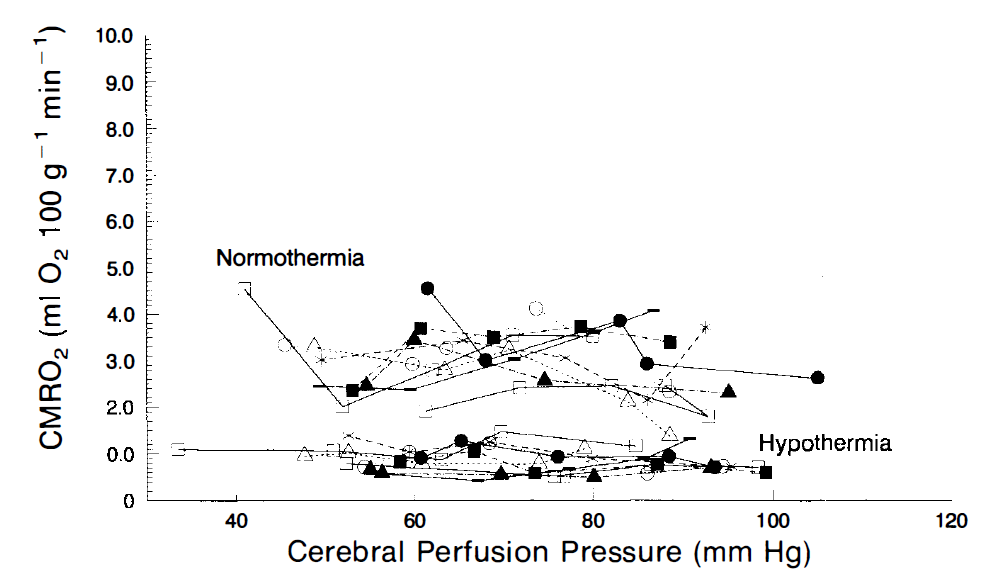
FIG.3. Raw data for CMRO2 versus CPP for the two temperature groups. There was no correlation between these two variables.
图 3. 两个温度组的 CMRO2 与 CPP 的原始数据。这两个变量之间没有关联性。
# 讨论
This study, in dogs, examined the cerebral pressure- flow relationship during CPB with α-stat acidbase management at normothermia (37°C) and moderate hypothermia (28°C). For tCBF and hCBF, we have shown that the autoregulatory plateau is not horizontal but has a finite positive slope at both temperatures studied. This contention is also supported from our finding that for both groups there was a decreased oxygen content difference (Art - SSS O2 content) as CPP increased at constant anesthetic depth (stable barbiturate anesthesia to an isoelectric EEG). These findings differ from previously published results examining cerebral autoregulation during CPB with moderate hypothermia and α-stat acid-base management (Govier et aI. , 1984; Murkin et aI., 1987; Aladj et aI., 1991). Clinically, preserved cerebral autoregulation is stated to be one of a number of reasons that the use of α-stat instead of pH-stat acid-base management is preferred for the conduct of CPB (Thomson, 1993). Our results for moderate hypothermia agree with those published by Greeley et aI. (1991) for more profound hypothermia.
这项研究在狗身上考察了在常温(37°C)和中度低温(28°C)下的 CPB 与 α-stat 酸碱管理的大脑压力 - 血流量关系。对于 tCBF 和 hCBF,我们已经表明,在所研究的两个温度下,自动调节平台不是水平的,而是有一个有限的正斜率。这一论点也从我们的发现中得到了支持,即在恒定的麻醉深度下(稳定的巴比妥酸盐麻醉到等电位脑电图),随着 CPP 的增加,两组的氧含量差(Art - SSS O2 含量)都有下降。这些发现与以前发表的研究 CPB 期间脑自动调节的结果不同,有适度低温和 α-stat 酸碱管理(Govier et aI. , 1984; Murkin et aI., 1987; Aladj et aI. , 1991)。在临床上,保留脑部自动调节是使用 α-stat 而不是 pH-stat 酸碱管理来进行 CPB 的原因之一(Thomson, 1993)。我们的中度低温结果与 Greeley et aI. (1991) 发表的更深度低温的结果一致。
The cause of our conflicting findings may relate to the fact that we examined autoregulation with a canine model and not in humans as in other studies. However, we feel our experimental design and the accompanying block-design analysis of covariance of our data permitted maximal statistical rigor for the investigation of whether cerebral autoregulation was preserved during α-stat CPB. In this study, CBF was measured multiple times using microsphere methodology, over a CPP range of 50-90 mmHg. We were able to tightly control other variables that could influence CBF such as hemoglobin concentration, PaCO2 and pH. Some workers have suggested that measurement of CBF during hypothermic CPB is critically time dependent as well (Prough et aI. , 1991; Rogers et aI., 1988). Hindman et aI. (1992) have recently suggested that the decrease in CBF seen during hypothermic CPB is a consequence of continued brain cooling. However, similar decreases in CBF have been shown by Warach et aI. (1987) in awake humans. Our model controlled for time-related effects by randomly allocating the five target CPP ranges (50-90 mmHg) in each experiment.
导致我们的研究结果相互矛盾的原因可能与我们用犬类模型而不是像其他研究那样在人类身上检查自动调节有关。然而,我们认为我们的实验设计和伴随的数据协方差分析允许最大的统计严谨性,以调查在 α-stat CPB 期间是否保留了大脑自动调节。在这项研究中,使用微球方法多次测量 CBF,CPP 范围为 50-90mmHg。我们能够严格控制可能影响 CBF 的其他变量,如血红蛋白浓度、PaCO2 和 pH。一些工作者认为,在低温 CPB 期间 CBF 的测量也是关键性的时间依赖(Prough et aI. , 1991; Rogers et aI. , 1988)。Hindman et aI. (1992) 最近提出,在低温 CPB 期间看到的 CBF 下降是持续脑部冷却的结果。然而,Warach 等人(1987 年)在清醒的人类中也显示了 CBF 的类似下降。我们的模型通过在每个实验中随机分配五个目标 CPP 范围(50-90mmHg)来控制与时间有关的影响。
We have demonstrated that the common slope (CPP as covariate) generated by a block-design analysis of covariance is statistically appropriate (lack of either a CPP x experiment effect or experiment effect when individual experiments were compared within each group). We feel that data that were analyzed in this fashion are reflective of how these experiments were done (multiple yet randomly determined CBF-CPP points). In addition, the p values were consistently lower with the data modeled in this fashion (Table 2). Note, however, that the linear regression analysis also indicates that a significant relationship exists between tCBF and hCBF versus CPP for both temperatures (p < 0.05 in each instance). But, our experimental design was such that pooling of data for our linear regression analysis differed from that usually undertaken. Five flow determinations per experiment, randomly allocated, may have controlled for some of the confounding variables that can influence consistent measurement of rCBF. Had we failed to control for other variables, including time as described above, nonsignificant linear regression analyses may have resulted. This is most evident for tCBF with hypothermia (p = 0.049). Data analyzed by linear regression analysis closely approximates the cut-off for statistical significance (p < 0.05), indicating CBF dependence on CPP (that is, impaired cerebral autoregulation) .
我们已经证明,由区块设计协方差分析产生的共同斜率(CPP 为协变量)在统计学上是合适的(当每组内的各个实验进行比较时,缺乏 CPP× 实验效应或实验效应)。我们认为,以这种方式分析的数据反映了这些实验是如何完成的(多个但随机确定的 CBF-CPP 点)。此外,以这种方式建模的数据,P 值一直较低(表 2)。然而,请注意,线性回归分析也表明,两个温度的 tCBF 和 hCBF 与 CPP 之间存在明显的关系(在每个实例中 p < 0.05)。但是,我们的实验设计是这样的,为我们的线性回归分析汇集的数据与通常进行的不同。每个实验的五个流量测定,随机分配,可能已经控制了一些可能影响 rCBF 一致测量的混杂变量。如果我们没有控制其他变量,包括上述的时间,可能会导致不显著的线性回归分析。这在体温过低的 tCBF 上最为明显(p = 0.049)。通过线性回归分析的数据接近统计学意义的临界点(p < 0.05),表明 CBF 对 CPP 的依赖性(即大脑自动调节功能受损)。
Examination of Fig. 1 suggests that tCBF is much more heterogeneous during normothermic than hypothermic bypass. In fact, a greater variance was seen for Group N by Bartlett s test for homogeneity of variances. A greater heterogeneity of CBF during normothermic bypass versus hypothermic bypass has recently been shown by others (Hindman et aI., 1992). King et al. (1985) state that the various factors contributing to the observed variance with the radioactive microsphere technique is the sum of contributing variances. These include spatial, methodologic, and temporal flow fluctuation variances. Which, if any, of these variances accounts for the differences between normothermic and hypothermic blood flow is not known. Regardless, less data scatter is evident in Group H. Reduced data scatter provides greater statistical power for linear regression analysis (by reducing the residual mean square, an estimate of experimental error; Steel and Torrie, 1960b) and may explain why impaired autoregulation has been previously noted with profound hypothermia but is not usually seen with moderate hypothermia (Greeley et aI., 1989; Taylor et aI., 1992).
对图 1 的研究表明,在常温分流过程中,tCBF 的异质性要比低温分流大得多。事实上,通过 Bartlett's 方差同质性测试,N 组的差异更大。最近其他人也证明了常温分流与低温分流期间 CBF 的更大异质性(Hindman et aI., 1992)。King 等人 (1985) 指出,造成放射性微球技术观察到的变异的各种因素是贡献变异的总和。这些因素包括空间、方法和时间上的流量波动变异。这些变异中的哪一个(如果有的话)是正常体温和低温血流之间差异的原因,目前还不清楚。不管怎么说,H 组的数据散点明显较少。数据散乱的减少为线性回归分析提供了更大的统计能力(通过减少残余均方,对实验误差的估计;Steel 和 Torrie,1960b),并可能解释为什么以前注意到深度低温时自动调节功能受损,但通常在中度低温时没有看到(Greeley 等,1989;Taylor 等,1992)。
For the cerebral hemisphere, a significantly steeper slope for the autoregulatory curve was seen with normothermia than with moderate hypothermia (p = 0.032). Thus, if these findings are applicable to the clinical situation, the brain is potentially at greater risk of ischemic damage during normothermic CPB as cerebral protection afforded by hypothermia and better preserved autoregulation to supratentorial structures are both lost. The difference in slopes approached statistical significance for tCBF as well (p = 0.059). That no temperaturedependent difference in slopes was evident for tCBF may be due to the fact that the autoregulatory slopes were independent of temperature for brain stem structures (p = 0.999). These results confirm a previous finding from this laboratory, viz., brain stem structures demonstrate a flatter cerebral pressure- flow relation than supratentorial structures (Patel and Mutch, 1990). This study indicates that the effect is independent of temperature.
对于大脑半球,常温下的自动调节曲线的斜率明显比中度低温下的陡峭(p = 0.032)。因此,如果这些发现适用于临床情况,那么在常温 CPB 期间,大脑有可能面临更大的缺血损伤风险,因为低温提供的大脑保护和保存较好的对上层结构的自动调节功能都会丧失。tCBF 的斜率差异也接近统计学意义(p = 0.059)。tCBF 的斜率没有明显的温度依赖性差异,这可能是由于脑干结构的自动调节斜率与温度无关(p = 0.999)。这些结果证实了本实验室以前的一个发现,即脑干结构比脑膜上结构表现出更平坦的大脑压力 - 血流量关系(Patel 和 Mutch,1990)。这项研究表明,这种影响是独立于温度的。
Our results indicate that the Q10 for dog cerebral cortex is 3.8. This is higher than most previously published results. Michenfelder and Theye (1968) found Q10 to be 2.43. In their study, Q10 was determined in six dogs by regression analysis of 10 data points over a 6°C temperature range. Rosomoff and Holaday (1954) found Q10 to be 3.3 from studies in four dogs. Bering (1974) found Q10 to be 3.4 in dogs over a temperature range from 37 to 19°C. Recent work from Lazenby et al. (1992) has demonstrated a canine Q10 varying between 3.73 and 4.11. Greeley et al. (1991) have recently demonstrated a Q10 of 3.65 in infants and children. This is significantly higher than previously reported values of 2.4-2.8 in humans (Croughwell et aI., 1991; Prough et al., 1991). Our data were derived from 44 and 45 determinations of CMRO2 in Group N and H, respectively. The high Q10 calculated in our study may result from a number of factors: (a) Our data are perhaps most representative of cerebral hemispheric Q10 (instead of total cerebral Q10) as we were able to correlate the arterial to SSS oxygen content difference for the cerebral hemisphere with matching measurements of hCBF using microsphere methodology; (b) the calculation of Q10 may have been affected due to indirect measurement of O2 contents with a Radiometer ABL-3 blood gas analyzer. With this blood gas analyzer, O2 content is calculated from the following formula: O2 content = 0.6206 x Hb x Sat + 0.00136 x PO2 mmol/L where 0.6206 = conversion factor for Hb concentration in mg% to mmol/L and 0.00136 = solubility coefficient for O2 in blood (mmol/L x mmHg). However, we have compared these calculated results for oxygen content in canine blood with directly measured oxygen content in canine blood using a Radiometer OSM3 (a hemoximeter). Correlations were very high (r2 = 0.87-0.97 with a consistently high offset independent of O2 saturation). These findings do not suggest a likely source of error for our calculation of Q10.
我们的结果表明,狗大脑皮层的 Q10 是 3.8。这比以前发表的大多数结果要高。Michenfelder 和 Theye(1968)发现 Q10 是 2.43。在他们的研究中,通过对 6℃温度范围内 10 个数据点的回归分析,确定了 6 只狗的 Q10。Rosomoff 和 Holaday(1954)通过对四只狗的研究发现 Q10 为 3.3。Bering (1974) 发现在 37 至 19℃的温度范围内,狗的 Q10 为 3.4。Lazenby 等人(1992 年)的最新研究表明,犬的 Q10 在 3.73 和 4.11 之间。Greeley 等人(1991 年)最近证明婴儿和儿童的 Q10 为 3.65。这明显高于以前报道的人类 2.4-2.8 的数值(Croughwell 等人,1991;Prough 等人,1991)。我们的数据分别来自 N 组和 H 组的 44 和 45 次 CMRO2 的测定。我们的研究中计算出的高 Q10 可能是由一些因素造成的。(a) 我们的数据也许最能代表大脑半球的 Q10(而不是总的大脑 Q10),因为我们能够用微球方法将大脑半球的动脉与 SSS 氧含量差异与 hCBF 的匹配测量联系起来;(b) Q10 的计算可能由于用 Radiometer ABL-3 血气分析仪间接测量 O2 含量而受到影响。用这种血气分析仪,O2 含量是按以下公式计算的。O2 含量 = 0.6206 x Hb x Sat + 0.00136 x PO2 mmol/L 其中 0.6206 = Hb 浓度(mg%)与 mmol/L 的转换系数,0.00136 = O2 在血液中的溶解度系数(mmol/L x mmHg)。然而,我们将这些犬类血液中氧含量的计算结果与使用 Radiometer OSM3(血氧仪)直接测量的犬类血液中氧含量进行了比较。相关性非常高(r2 = 0.87-0.97,与 O2 饱和度无关的偏移量一直很高)。这些发现并不表明我们在计算 Q10 时可能存在误差。
Our measurement of Q10 was based on the CMRO2 ratio from two groups of animals both on CPB. By controlling for time-related effects we feel our Q10 measurements for CPB are stable. The CMRO2 in the normothermic group had a range of 2.8 ± 0.8 to 3.1 ± 0.8 ml 02100 g- I min - l over the five microsphere injection periods. In the hypothermic group, CMRO2 was 0.8 ± 0.2 to 0.3 ml O2 100 g-1 min-1 for all five injection periods. That time may have an effect on the determination of Q10 during CPB is evident from the study of the data of Greeley et aI. (1991). Following 5 min of stable hypothermic bypass, the ratio of CMRO2 values at 28 and 19°C in two similar groups of patients was 0.63:0.16-a Q10 of 4.6. When the same two groups are compared after 25 min of bypass, the ratio of CMRO2 values at 28 and 20°C was 0.94:0.39-a Q10 of 3.0. A similar time effect has been observed by Lazenby et aI. (1992) such that brain Q10 values decreased with time. These changes in Q10 over time may relate to continued cooling of the brain as indicated in the work by Hindman et aI. (1992). Our measurements of Q10 are also felt to be stable because our metabolic data comparing the two temperatures were at stable deep barbiturate anesthesia (EEG isoelectricity). Thus, the CMRO2 ratio is purely a consequence of the metabolic depression seen with decreasing temperature (Steen et aI., 1983). The effect of temperature on volatile agent partial pressure has been eliminated.
我们对 Q10 的测量是基于两组都在 CPB 上的动物的 CMRO2 比率。通过控制与时间有关的影响,我们觉得我们对 CPB 的 Q10 测量是稳定的。常温组的 CMRO2 在五个微球注射期的范围为 2.8±0.8 至 3.1±0.8 ml O2 100 g-1 min-1。在低温组中,CMRO2 在所有五个注射期中为 0.8±0.2 至 0.3 ml O2 100 g-1 min-1。时间可能对 CPB 期间 Q10 的确定有影响,这一点从 Greeley 等人(1991)的数据研究中可以看出。在稳定的低温分流 5 分钟后,两组相似的病人在 28 和 19℃时的 CMRO2 值之比为 0.63:0.16-Q10 为 4.6。当同样的两组患者在分流 25 分钟后进行比较,在 28 和 20°C 时 CMRO2 值的比值为 0.94:0.39-Q10 为 3.0。Lazenby et aI. (1992) 也观察到类似的时间效应,如大脑 Q10 值随着时间的推移而下降。这些 Q10 随时间的变化可能与 Hindman et aI. (1992) 的工作中指出的大脑持续冷却有关。我们对 Q10 的测量也被认为是稳定的,因为我们比较两个温度的代谢数据是在稳定的巴比妥酸盐深度麻醉下(EEG 等电)。因此,CMRO2 比率纯粹是随着温度的降低而出现的代谢抑制的结果(Steen et aI., 1983)。温度对挥发性药剂分压的影响已被消除。
In a broader context, this experiment represents an attempt to study cerebral autoregulation by altering CPP independently of the effects of pharmacologic intervention. As CPP was altered exclusively by changes in perfusion flow rate, we avoided administration of vasopressors or vasodilators- agents known to independently alter CBF (Patel and Mutch, 1990; Reynier-Rebuffel et aI., 1987; Tabaddor et aI., 1977; Tuor and McCulloch, 1986). This study suggests that nonpulsatile CPB with α-stat management alters the ability of the cerebral circulation to auto regulate irrespective of temperature. Others have noted that in certain circumstances CPB affects cerebral flow-metabolic coupling (Greeley et aI., 1993). Such uncoupling could potentially influence cerebral autoregulation. Whether pulsatile CPB would have resulted in retained cerebral autoregulation with a block design analysis of covariance of CBF-CPP data is an interesting but untested hypothesis. Regardless, this study indicates that the experimental design and statistical analysis can influence the interpretation of whether cerebral autoregulation is intact.
在更广泛的背景下,本实验代表了通过改变 CPP 独立于药物干预的影响来研究大脑自动调节的尝试。由于 CPP 完全由灌注流速的变化而改变,我们避免了血管抑制剂或血管扩张剂的管理 -- 已知可独立改变 CBF 的药剂(Patel 和 Mutch,1990;Reynier-Rebuffel 等人,1987;Tabaddor 等人,1977;Tuor 和 McCulloch,1986)。这项研究表明,非脉冲式 CPB 与 α-stat 管理改变了脑循环的自动调节能力,而不考虑温度。还有人指出,在某些情况下,CPB 会影响脑血流 - 代谢耦合(Greeley et aI., 1993)。这种解耦有可能影响脑的自动调节。脉冲式 CPB 是否会导致 CBF-CPP 数据的方差分析保留脑自律调节,这是一个有趣但未经测试的假设。无论如何,这项研究表明,实验设计和统计分析可以影响对脑自律调节是否完整的解释。
In conclusion, we have used a canine model to study the cerebral pressure-flow relationship during α-stat CPB. This model has enabled us to rigorously demonstrate that CBF is dependent on CPP, that is, the autoregulatory plateau is not horizontal during CPB but has a positive slope during both normothermia and moderate hypothermia, during deep barbiturate anesthesia. Assumptions inherent in pooling of CBF data from multiple subjects are eliminated by our data analysis. Cerebral hemispheric oxygen requirements, while on CPB, demonstrated a Q10 of 3.8 with this model. Possible explanations for the high value for Q10 are discussed.
总之,我们使用了一个犬类模型来研究 α-stat CPB 期间的大脑压力 - 血流量关系。这个模型使我们能够严格地证明 CBF 依赖于 CPP,也就是说,在 CPB 期间,自动调节平台不是水平的,而是在常温和中度低温期间,在深巴比妥酸盐麻醉期间有一个正的斜率。我们的数据分析消除了将多个受试者的 CBF 数据汇集在一起的固有假设。大脑半球的氧气需求,在 CPB 时,用这个模型显示的 Q10 为 3.8。我们讨论了对 Q10 高值的可能解释。
# 附录
The experiments were of a repeated measures design. Animals were randomly allocated to the hypothermic or normothermic groups. Then the animals were randomly allocated to each of five target CPP s and the corresponding rCBF determined. The relationship between CPP and rCBF under the two temperature conditions were analyzed with a block design analysis of covariance (ANCOVA). The approach was not to adjust for the covariate but rather to compare the regression lines or slopes. The model can be described as:
实验采用了重复测量设计。动物被随机分配到低体温组或常温组。然后将动物随机分配到五个目标 CPPs 中的每一个,并确定相应的 rCBF。在两种温度条件下,CPP 和 rCBF 之间的关系用区块设计的协方差分析(ANCOVA)进行分析。该方法不是为了调整协变量,而是为了比较回归线或斜率。该模型可以描述为。
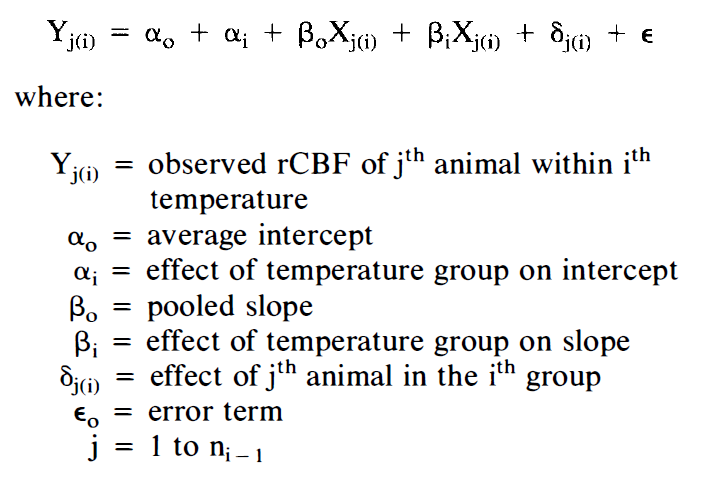
However, when we found that the slopes were not parallel (βi term; p <0.05) we separately analyzed the CPP-rCBF relationship for the two temperature groups. The model used is described as:
然而,当我们发现斜率不平行时(βi 项;p <0.05),我们分别分析了两个温度组的 CPP-rCBF 关系。所用的模型描述为。