
 人脑的血流与氧耗
人脑的血流与氧耗
# 人脑的血流与氧耗
Cerebral Blood Flow and Oxygen Consumption in Man
NIELS A. LASSEN1
Laboratory of Clinical Science, National Institute of Mental Health, National Institutes of Health, Bethesda, Maryland
人脑的血流与氧耗
NIELS A. LASSEN1
临床科学实验室,国家心理健康研究所,国家卫生研究院,马里兰州贝塞斯达
# 序言
The blood flow and oxygen metabolism of the human brain has been studied intensively since Kety developed the inert gas method in 1945. More than 200 clinical studies employing this method have been published so far, and now the former terra incognita is well mapped out. The information gained from all these studies will form the subject of the present review. It will also include, however, the results obtained by an indicator injection technique which has been applied to the measurement of cerebral blood flow in man to a much more limited extent. The early results obtained in this particular field have been reviewed by Schmidt (292) and Kety (156-163) and by other authors (38, 61, 76, 216, 281, 307). The aim of the present review is to offer an up to date presentation of the subject, and, in particular, to discuss certain aspects in greater detail. The general field of cerebral circulation was reviewed by Wolff in 1936 (348), by many authors in a comprehensive study in 1938 (41), and extensive bibliographic compilations of original contributions from 1938 to 1952 have also been published (255, 256). The pharmacology of the cerebral circulation alone, which has recently been reviewed by Sokoloff (318), forms an overwhelming body of knowledge. In the present study great emphasis will be put on information regarding cerebral oxygen consumption in man, whereas only scant attention will be paid to the intermediary metabolism of the brain. Himwich in 1951 published an excellent review (142) of much of the pertinent literature in this rapidly expanding field. Reference is also made to the recent study by Sokoloff (319).
自从 Kety 于 1945 年开发出惰性气体方法以来,人们对人脑的血流和氧代谢进行了深入研究。迄今为止,已经发表了 200 多项采用这种方法的临床研究,现在已经很好地描绘了以前的未知领域。从所有这些研究中获得的信息将构成本次审查的主题。然而,它也将包括通过指示剂注射技术获得的结果,该技术已在更有限的范围内应用于人类脑血流量的测量。 Schmidt (292) 和 Kety (156-163) 以及其他作者 (38, 61, 76, 216, 281, 307) 回顾了在这一特定领域获得的早期结果。本综述的目的是提供对该主题的最新介绍,特别是更详细地讨论某些方面。 Wolff 于 1936 年回顾了脑循环的一般领域 (348),许多作者在 1938 年的一项综合研究中回顾了 (41),并且还出版了 1938 年至 1952 年原始贡献的大量书目汇编 (255, 256)。 Sokoloff(318)最近对脑循环的药理学进行了综述,形成了压倒性的知识体系。在本研究中,将重点关注有关人类脑耗氧量的信息,而很少关注大脑的中间代谢。 Himwich 于 1951 年发表了一篇关于这个迅速发展的领域中许多相关文献的优秀评论 (142)。还可以参考 Sokoloff (319) 最近的研究。
The first attempt to measure the cerebral blood flow in man was made in 1941 by observing the displacement of spinal fluid caused by compression of the two jugular veins (74). This method, however, was based upon assumptions whose validity must be seriously questioned (315). Better methods are now available: the inert gas method (170) and the indicator injection method (110). These two methods also permit measurement of the cerebral oxygen uptake. The inert gas method is presumably the most accurate, and it is at the same time technically the less complicated of the two methods. Therefore it is not surprising that it has won wide acceptance and that it has been the method of choice for the study of the cerebral circulation in man.
1941 年,通过观察压迫两条颈静脉引起的脊髓液位移,首次尝试测量人的脑血流量(74)。然而,这种方法是基于假设,其有效性必须受到严重质疑(315)。现在有了更好的方法:惰性气体法(170)和指标注射法(110)。这两种方法也允许测量脑氧摄取量。惰性气体法可能是最准确的,同时在技术上也是这两种方法中最不复杂的。因此,它赢得了广泛的认可,成为研究人类脑循环的首选方法也就不足为奇了。
# 惰性气体法
Inert Gas Method
The inert gas method is based on the Fick Principle (79). This principle represents a practical application of the law of conservation of matter to the problem of blood flow measurements. Regarding the inert gas method, the Fick Principle may be phrased: Blood flow to any organ or to the body as a whole may be obtained as the ratio between the uptake of inert gas per unit time and the arteriovenous inert gas difference across the organ in question. Kety and Schmidt developed the inert gas method and applied it to the study of cerebral circulation in man (155, 170, 173). Although the method has since been successfully adapted for the measurement of blood flow in other organs in man, as well as in various experimental animals, human cerebral blood flow measurements have remained the most important application of the inert gas method. The procedure may be briefly described as follows: An inert gas is introduced into the arterial blood supply of the brain via the lungs. During a suitable period of inhalation of a constant concentration of the gas, blood samples are taken from a peripheral artery—assumed to be representative of the cerebral arteries—and from the main venous drainage from the brain, the internal jugular vein. After a suitable experimental period ensuring a fair degree of saturation of all cerebral tissues, it is possible to estimate indirectly the inert gas uptake per unit weight of brain from the venous concentration. But it is not possible in this way to estimate the inert gas uptake in the total brain. For this reason the inert gas method does not measure total cerebral blood flow but the flow per unit weight of the brain. The unit of brain weight referred to is usually 100 gm. Therefore, in the following discussion, the abbreviation CBF will be taken to mean the cerebral blood flow per 100 gm of brain per minute. The CMRO2 is the cerebral metabolic rate of oxygen calculated by multiplying the CBF and the corresponding arteriovenous oxygen difference. The unit of CMRO2 is cc of O2 consumed per 100 gm of brain per minute.
惰性气体法是基于菲克原理(79)。该原理代表了物质守恒定律在血流测量问题上的实际应用。关于惰性气体法,菲克原理可以这样表述。任何器官或整个身体的血流量都可以通过单位时间内惰性气体的吸收量与横跨有关器官的动静脉惰性气体差值之间的比率来获得。Kety 和 Schmidt 开发了惰性气体方法,并将其应用于人类脑循环的研究(155,170,173)。尽管此后该方法被成功地应用于人类其他器官以及各种实验动物的血流测量,但人类脑血流测量仍然是惰性气体方法最重要的应用。该程序可简要描述如下。一种惰性气体通过肺部被引入大脑的动脉血液供应中。在吸入恒定浓度的气体的适当时期,从外周动脉 -- 被认为是代表脑动脉 -- 和从大脑的主要静脉引流 -- 颈内静脉 -- 采集血样。经过适当的实验期,确保所有的脑组织达到相当程度的饱和,就有可能从静脉浓度中间接估计出每单位重量的脑的惰性气体吸收量。但是不可能通过这种方式来估计全脑的惰性气体吸收量。由于这个原因,惰性气体方法并不测量总的脑血流量,而是测量每单位脑重量的流量。所指的脑重量单位通常是 100 克。因此,在下面的讨论中,CBF 的缩写将被理解为每分钟每 100 克大脑的脑血流量。CMRO2 是由 CBF 和相应的动静脉氧差相乘而计算出的脑部氧代谢率。CMRO2 的单位是每 100 克大脑每分钟消耗的氧气毫升。
The original technique (173) employed 15% N2O as the inert gas and a 10-minute inhalation period. During this period, five samples were taken from a peripheral artery and five from one of the internal jugular veins. Several minor modifications have been introduced: The continuous sampling technique of Schein-berg and Stead (284) reduced the number of blood samples necessary, but it probably also reduced the accuracy of the method; the volume of the blood samples has been reduced for the adaptation of the method for studies in children (11, 99, 152, 153); the use of Kr85 (a /3-emitting isotope of krypton) as the inert gas, increasing the number of blood samples, and sampling from both internal jugular veins, have resulted in some gain in precision (188, 234). A more fundamental modification has recently been developed by Lewis and associates, using the 7-emitting Kr79 as the inert gas (197, 198). By direct and continuous external measurement of the amount of inert gas in the whole brain and simultaneous blood sampling, it is possible to calculate the total cerebral blood flow and to follow any fairly rapid changes in this flow.
最初的技术(173)采用 15% 的 N2O 作为惰性气体,吸入时间为 10 分钟。在此期间,从外周动脉采集五个样本,从一个颈内静脉采集五个样本。已有一些小的修改。Schein-berg 和 Stead (284) 的连续采样技术减少了必要的血样数量,但可能也降低了该方法的准确性;为了适应儿童研究,减少了血样的体积(11,99,152,153);使用 Kr85(氪的一种 / 3 发射的同位素)作为惰性气体,增加血样数量,以及从两个颈内静脉采样,使精确度得到一些提高(188,234)。最近,Lewis 和他的同事开发了一个更基本的修改,使用 7 发射的 Kr79 作为惰性气体(197,198)。通过直接和连续的外部测量整个大脑中的惰性气体量,并同时进行血液采样,就可以计算出总的脑血流量,并跟踪这一流量的任何相当快速的变化。
The inert gas method is based upon a number of assumptions. These will be discussed with special regard to the different modifications. It will become apparent that some of the assumptions are only approximately correct. For this reason it is of considerable importance that the validity of the method has been clearly demonstrated by Kety and Schmidt (170, 173). These authors found a good agreement between the inert gas method and direct blood flow measurements in nine monkey experiments covering a large span of perfusion values (CBF values from 17 to 76 cc/100gm/min.).
惰性气体法是建立在一些假设之上的。我们将讨论这些假设,并特别考虑到不同的修改。很明显,有些假设只是近似正确。由于这个原因,Kety 和 Schmidt(170,173)已经明确证明了该方法的有效性,这一点相当重要。这些作者在九个猴子实验中发现惰性气体方法和直接血流测量之间有很好的一致性,涵盖了大范围的灌注值(CBF 值从 17 到 76 毫升 / 100gm/min.)。
# 惰性气体的选择
Choice of Inert Gas
It is assumed that the inert gas employed does not influence the CBF and CMRO2. In nearly all clinical studies 15% N2O has been used as described by Kety and Schmidt (170, 173). Usually the subjects feel a slight tingling in the hands and feet, and often they become somewhat drowsy. It thus appears that even in as low a concentration as 15 % nitrous oxide is not completely devoid of cerebral effects. When radioactive isotopes are employed, the concentration of the inert tracer is infinitesimally small and there is no evidence of cerebral effects. The normal values determined by the original N2O method (173) are almost identical with those obtained much later by the Kr86 modification (188). This demonstrates that 15% N2O does not significantly affect the CBF and CMRO2. The choice of inert gas depends on the analytical problems and on the nature of the physiological situation which is to be studied. The 15% N2O is easy to administer and analyze, and for many kinds of studies the accuracy obtained is sufficient. Employment of radioisotopes allows a highly specific, accurate and rapid analysis, which can readily be adapted for handling a large number of samples per study (188, 197, 198). Such techniques permit the reduction of random experimental errors (234). Gamma-emitting inert gases allow, as already stated, the study of rapid changes in total cerebral blood flow (197, 198).
假设采用的惰性气体不影响 CBF 和 CMRO2。如 Kety 和 Schmidt(170,173)所述,几乎所有的临床研究都使用了 15% 的 N2O。通常受试者会感到手和脚有轻微的刺痛,而且经常会变得有些昏昏欲睡。由此看来,即使浓度低至 15% 的一氧化二氮也并非完全没有脑部影响。当使用放射性同位素时,惰性示踪剂的浓度极小,没有证据表明对大脑有影响。由最初的 N2O 方法(173)确定的正常值与后来由 Kr86 修改得到的正常值几乎相同(188)。这表明 15% 的 N2O 并不明显影响 CBF 和 CMRO2。惰性气体的选择取决于分析问题和要研究的生理情况的性质。15% 的一氧化二氮很容易管理和分析,而且对于许多类型的研究来说,所获得的准确性是足够的。使用放射性同位素可以进行高度特异性、准确和快速的分析,可以很容易地适用于处理每项研究的大量样品(188,197,198)。这种技术允许减少随机实验误差(234)。如前所述,伽马射线惰性气体允许研究总脑血流的快速变化(197,198)。
# 惰性气体在大脑和血液中的溶解度
Solubility of Inert Gases in Brain and Blood
The ratio of the solubility of the inert gas in brain and whole blood is a factor necessary for calculating cerebral blood flow. Both N2O and Kr85 are somewhat more soluble in red cells than in plasma (167, 188). Hence it follows that the whole blood solubility and, therefore, also the above mentioned ratio, varies to some extent with the hematocrit value. In pronounced cases, variations of about 10 per cent can be calculated (167, 188). When comparing groups of subjects with different hematocrit levels, omission of correction for this factor may thus be expected to cause a moderate systematical error of CBF and CMRO2. No correction for the influence of variations of the hematocrit has been used in studies employing the N2O technique, whereas such a correction has been applied by Lassen and Munck when developing the Kr85 modification (188).
惰性气体在大脑和全血中的溶解度之比是计算脑血流量的一个必要因素。一氧化二氮和 Kr85 在红细胞中的溶解度都比在血浆中的溶解度大一些(167,188)。因此,全血的溶解度以及上述比率在一定程度上随血细胞比容值的变化而变化。在明显的情况下,可以计算出大约 10% 的变化(167,188)。当比较不同血细胞比容水平的受试者群体时,忽略对这一因素的校正可能会导致 CBF 和 CMRO2 的适度系统误差。在采用 N2O 技术的研究中,没有对血细胞比容变化的影响进行校正,而 Lassen 和 Munck 在开发 Kr85 模型时则采用了这种校正(188)。
Individual variations in the solubility of inert gases in the brain are presumably quite small. N2O studies demonstrated the same solubility in pathological brain tissue as in normal human and canine brain (167). The absolute value of the brain-blood partition coefficient is of much less importance for the method than its constancy. The experimental procedures employed in determining this coefficient for N2O and Kr85 have inherent technical difficulties which could tend to give somewhat low values (167, 188). For N2O the coefficient was found to be 1.00 (167) and for Kr85, 1.06 for a hematocrit of 50% (188). Simultaneous N2O and Kr79 studies have confirmed that the ratio of the coefficients is close to 1.00/1.06 (197). When y-emitting inert gases are used, the calculation of the total cerebral blood flow and oxygen uptake is independent of the solubility in brain and blood (197)-
惰性气体在大脑中的溶解度的个体差异可能相当小。一氧化二氮的研究表明,其在病理脑组织中的溶解度与在正常人和犬脑中的溶解度相同(167)。脑 - 血分配系数的绝对值对该方法的重要性远远低于其恒定性。在确定 N2O 和 Kr85 的这一系数时采用的实验程序存在固有的技术困难,可能会给出较低的数值(167,188)。对于一氧化二氮,该系数被发现为 1.00(167),对于 Kr85,在血细胞比容为 50% 时,该系数为 1.06(188)。同时进行的 N2O 和 Kr79 的研究证实,系数的比率接近 1.00/1.06(197)。当使用 y 发射的惰性气体时,总脑血流量和摄氧量的计算与大脑和血液中的溶解度无关 (197)-
# 异质性脑灌注的影响 2
Effect of Heterogeneous Cerebral Perfusion2
When calculating the CBF according to the equation of Kety and Schmidt (173), it is assumed that at the end of the experiment the average inert gas tension of the brain is the same as the tension of the mixed cerebral venous blood. For each separate cerebral tissue and its corresponding venous blood this relation holds true, as diffusion equilibrium is almost instantaneous according to theoretical calculations by Copperman, cited by Kety (159). However, as the various cerebral tissues have different perfusion rates (95, 164), this obviously does not apply for the brain as a whole before all cerebral tissues are in diffusion equilibrium with the arterial inert gas tension. Thus, ideally, the experiment should be carried on until all cerebral tissues are completely saturated, as recently reemphasized by Sapirstein and Ogden (269). In practice, however, it is only important that the assumption is approximately fulfilled. Like Kety and Schmidt (170, 173)> nearly all investigators have used an experimental duration of 10 minutes. The choice of 10 minutes was based on theoretical considerations (170) and on animal experiments where direct comparison was made between the N2O concentrations of the whole brain and the mixed cerebral venous blood (167). External y-ray measurement of the cerebral uptake of radioactive inert gases in man gave confirmatory evidence (157).
根据 Kety 和 Schmidt(173)的公式计算 CBF 时,假定在实验结束时,大脑的平均惰性气体张力与混合脑静脉血的张力相同。对于每个独立的脑组织及其相应的静脉血来说,这种关系是成立的,因为根据 Kety(159)引用的 Copperman 的理论计算,扩散平衡几乎是瞬间的。然而,由于各种脑组织有不同的灌注率(95,164),在所有脑组织与动脉惰性气体张力达到扩散平衡之前,这显然不适用于整个大脑。因此,理想情况下,实验应该进行到所有脑组织完全饱和为止,这一点最近由 Sapirstein 和 Ogden(269)再次强调。然而,在实践中,这个假设被近似地实现才是重要的。像 Kety 和 Schmidt(170,173)> 一样,几乎所有的研究者都采用了 10 分钟的实验时间。选择 10 分钟是基于理论考虑(170)和动物实验,在动物实验中对全脑和混合脑静脉血的 N2O 浓度进行了直接比较(167)。对人脑吸收放射性惰性气体的外部 Y 射线测量给出了证实的证据(157)。
When the CBF is calculated serially for each minute, as recommended by Kety and Schmidt (173), it becomes apparent that the CBF value does not reach a constant minimal value at 10 minutes. The calculated CBF continues to decrease beyond 10 minutes, although a marked leveling-off of values is usually noted. This observation indicates that the effect of heterogeneous perfusion is also present to a small degree at 10 minutes. Kety and Schmidt were originally of the opinion that the cerebral perfusion was so rapid that even the areas of slowest perfusion
当按照 Kety 和 Schmidt (173) 的建议,连续计算每分钟的 CBF 时,就会发现 CBF 值在 10 分钟时并没有达到一个恒定的最小值。计算出的 CBF 在 10 分钟后继续下降,尽管通常会注意到数值的明显平缓。这一观察表明,异质性灌注的影响在 10 分钟时也存在,但程度不大。Kety 和 Schmidt 最初认为,脑灌注是如此之快,甚至是灌注最慢的区域
2 Strictly speaking the term, heterogeneous cerebral clearance rate of gases, should be used, as the proper exponential coefficients are ratios of both perfusion and relative solubility (159). The relative solubility of inert gases in different areas of the brain varies much less than the perfusion rates (95), and for this reason it was felt justified to use the term, heterogeneous cerebral perfusion, as it is much easier to conceptualize.
2 严格来说,应该使用 "异质性脑气体清除率" 这一术语,因为适当的指数系数是灌注和相对溶解度的比率(159)。惰性气体在大脑不同区域的相对溶解度的变化要比灌注率小得多(95),由于这个原因,我们认为有理由使用异质性脑灌注这个术语,因为它更容易概念化。
were in equilibrium with the mixed cerebral venous blood after io minutes. For this reason they attributed the continued decrease of the calculated CBF to extracerebral contamination (173). Lassen and Munck interpreted the same phenomenon differently (188). They held the opinion that some intracerebral tissue might have a relatively slow perfusion rate. The slow saturation of inert gas in such a tissue could cause the observed phenomenon. An attempt was made to take into account this slow component of supposedly cerebral origin. The duration of the experiment was extended to about 14 minutes, and a procedure of extrapolation to infinite time employed.
在 10 分钟后,脑血流与混合脑静脉血处于平衡状态。出于这个原因,他们将计算的 CBF 持续下降归因于脑外污染(173)。Lassen 和 Munck 对同一现象有不同的解释(188)。他们认为一些脑内组织可能有相对缓慢的灌注率。在这样的组织中,惰性气体的缓慢饱和可能导致观察到的现象。他们试图将这种据说是脑部的缓慢成分考虑在内。实验的持续时间被延长到大约 14 分钟,并采用了一个推断到无限长的程序。
Recent animal experiments by Kety and associates (164) have tended to resolve this question. These studies show that the white matter of the brain has a rather slow uptake rate of inert gases—so slow that it may well account for the fraction of the jugular blood which only slowly reaches the arterial inert gas concentration. Inserting the perfusion rates determined experimentally in normal unanesthetized cats (164) in the equations of Kety (159), it can be calculated that the inert gas tension of the whole brain reaches, in 10 minutes, about 90 per cent of the simultaneous inert gas tension of the mixed cerebral venous blood. In normal man the CBF value calculated at 10 minutes is thus at most about 10 per cent higher than the true value.
Kety 和他的同事们最近进行的动物实验(164)倾向于解决这个问题。这些研究表明,大脑白质对惰性气体的吸收率相当慢 -- 慢到很可能说明颈部血液中只有一部分缓慢达到动脉惰性气体浓度。将实验中确定的正常未麻醉猫的灌注率(164)插入 Kety(159)的方程式中,可以计算出整个大脑的惰性气体张力在 10 分钟内达到混合脑静脉血的同时惰性气体张力的 90% 左右。因此,在正常人中,10 分钟计算出的 CBF 值最多比真实值高 10% 左右。
The discussion in the present section is confined to the average case in which no significant extracerebral contamination of the cerebral venous blood sampled occurs (see below). It is concluded that due to heterogeneous cerebral perfusion, the 1 o-minute CBF value is always moderately higher than the true value. In subjects with high perfusion rates of all cerebral tissues the error is relatively small. A somewhat greater error is to be expected in subjects with subnormal CBF, with intracranial arteriovenous shunts or with an arterial inert gas curve which continues to rise at an unusual rate. Inserting fairly extreme values in the proper equations (159), it becomes apparent that the error in such cases is not likely to exceed 25 per cent. Thus, the effect of heterogeneous cerebral perfusion would not seriously invalidate the inert gas method. Apparently, no major conclusion on the blood flow and oxygen uptake of the human brain has been in error for this reason.
本节的讨论仅限于脑静脉血采样没有发生明显脑外污染的平均情况(见下文)。结论是,由于脑灌注的异质性,10 分钟的 CBF 值总是适度高于真实值。在所有脑组织高灌注率的受试者中,误差相对较小。在 CBF 不正常、有颅内动静脉分流或动脉惰性气体曲线以不正常速度持续上升的受试者中,预计误差会更大一些。在适当的方程式中插入相当极端的数值(159),就会发现在这种情况下的误差不可能超过 25%。因此,异质性脑灌注的影响不会使惰性气体法严重失效。显然,关于人脑的血流和摄氧量的主要结论都没有因为这个原因而出现错误。
# CBF 的恒定性
Constancy of CBF
When calculating the CBF, it is assumed that the cerebral perfusion does not change during the experiment. In order to obtain constant experimental conditions, the study is usually not started until about 15 minutes have elapsed after the vessels have been punctured. Repeated examinations of CBF under essentially unchanged conditions and with an interval of 30-40 minutes have been reported by many investigators (21, 128, 188, 199, 217; see also 20, 62, 146, 173, 270, 272, 282, 310, 321). These many reports, comprising over 100 studies, have shown that in the majority of cases no significant change of CBF occurs. Thus there is ample support for the conclusion that under supposedly steady state conditions the CBF does not usually vary materially within the 10-15 minute sampling period.
在计算 CBF 时,假设脑灌注在实验中不发生变化。为了获得恒定的实验条件,通常在血管穿刺后约 15 分钟后才开始研究。许多研究者报告了在基本不变的条件下,间隔 30-40 分钟重复检查 CBF(21, 128, 188, 199, 217;另见 20, 62, 146, 173, 270, 272, 282, 310, 321)。这些由 100 多项研究组成的许多报告表明,在大多数情况下,CBF 没有发生明显变化。因此,有充分的证据表明,在所谓的稳态条件下,CBF 在 10-15 分钟的采样期内通常没有实质性的变化。
It will become apparent in the section on the regulation of CBF, that minor changes in the pulmonary ventilation and the ensuing changes in the arterial carbon dioxide tension must be considered the most likely cause of CBF variations in supposedly steady state conditions. It has been demonstrated experimentally that the cerebral arteriovenous oxygen difference, (A-V)O2, varies inversely with CBF in hyper- and hypocapnia, so that the CMRO2 is unchanged (171, 174). This implies that the demonstration of constancy of (A-V)O2 during an individual experiment would, under many conditions, constitute strong evidence of the constancy of CBF. The CBF is proportional to the area between the cerebral arterial and venous inert gas saturation curves. As the main part of this area is determined during the first few minutes of the experiment, it is preferable to calculate the CMRO2 from an (A-V)O2 obtained during the first few minutes. In case minor variations of CBF and (A-V)O2 should occur, this procedure would tend to minimize the effect on the CMRO2. The use of gamma-emitting inert gases makes it possible to measure fairly rapid changes in total cerebral blood flow continuously over a period of about 5 minutes (197).
在 CBF 的调节一节中可以看出,肺通气的微小变化和随之而来的动脉二氧化碳张力的变化必须被认为是在所谓的稳态条件下 CBF 变化的最可能原因。实验证明,在高碳酸血症和低碳酸血症中,脑动脉血氧差(A-V)O2 与 CBF 成反比,因此 CMRO2 是不变的(171,174)。这意味着,在许多条件下,在个别实验中证明 (A-V) O2 的恒定性将构成 CBF 恒定的有力证据。CBF 与大脑动脉和静脉惰性气体饱和度曲线之间的面积成正比。由于该面积的主要部分是在实验的头几分钟内确定的,因此最好是根据头几分钟内获得的(A-V)O2 来计算 CMRO2。如果 CBF 和 (A-V) O2 发生微小的变化,这个程序会使对 CMRO2 的影响最小化。使用伽马射线惰性气体可以在大约 5 分钟内连续测量总脑血流的快速变化(197)。
# 脑动脉血
Cerebral Arterial Blood
Peripheral arterial blood is usually assumed to be representative of cerebral arterial blood, and only a few investigators use blood samples from the carotid artery (27). Superimposable saturation curves were found in a few experiments where blood was sampled simultaneously from the carotid and femoral arteries (150, 178). In special cases, such as congenital heart diseases, peripheral arterial blood might differ from cerebral arterial blood.
周围动脉血通常被认为是代表脑动脉血的,只有少数研究者使用颈动脉的血样(27)。在少数同时从颈动脉和股动脉取血的实验中,发现了可叠加的饱和度曲线(150,178)。在特殊情况下,如先天性心脏病,外周动脉血可能与脑动脉血不同。
# 颈内动脉血的脑外污染
Extracerebral Contamination of Internal Jugular Blood
Blood supposedly sampled from the superior bulb of the internal jugular vein is assumed to be cerebral venous blood essentially free from extracerebral contamination. The technique for puncturing the vein at this high level is well described (106, 236), and in actual practice it is not unusual that the base of the skull is encountered by the needle before the correct position is found. Fazekas and associates found that by inserting the needle a little further spinal fluid could be withdrawn (6, 32). Clearly in these cases the needle must have penetrated the jugular foramen and entered the cranial cavity. Thus it seems unlikely that blood from the facial vein contaminates the venous samples in the average case when the standard technique is employed. This conclusion is also supported by the result of dye injection studies by Shenkin, Harmel and Kety (306), who found that the blood in the superior bulb of the internal jugular vein contains very little blood derived from the external carotid artery. Comparing the dye concentration in the internal jugular to that in the external jugular, a value for extracerebral admixture was calculated. The maximal value of this admixture was 6.6 per cent and the average value 2.7 per cent. These low values may, however, be somewhat too high. By the method of calculation employed, the authors cautiously made two assumptions, both of which tended to exaggerate the calculated value of the contamination. Thus, it was assumed that no branches of the external carotid artery supplied blood to cerebral tissue and, also, that the extracerebral admixture was caused by blood as diluted with respect to dye as the external jugular blood. An admixture of the calculated value of a few percentages cannot affect the CBF seriously. Thus it is to be concluded that in the average case no gross extracerebral contamination of the internal jugular blood occurs, and thus the CBF refers essentially to the intracranial tissues, i.e., mainly the brain.
据称从颈内静脉上球部取的血被认为是脑静脉血,基本上不受脑外污染。在这一高位穿刺静脉的技术已经有了很好的描述(106,236),在实际操作中,在找到正确位置之前,针头碰到颅底是很正常的。Fazekas 和他的同事发现,将针头再往前插一点就可以抽出脊髓液(6,32)。显然,在这些病例中,针头肯定已经穿透了颈椎孔,进入了颅腔。因此,在采用标准技术的情况下,面部静脉的血液似乎不太可能污染普通的静脉样本。Shenkin、Harmel 和 Kety(306)的染料注射研究结果也支持这一结论,他们发现颈内静脉上球部的血液中很少有来自颈外动脉的血液。将颈内静脉中的染料浓度与颈外静脉中的染料浓度相比较,计算出一个脑外混合的数值。这种混杂物的最大值为 6.6%,平均值为 2.7%。然而,这些低值可能有些过高。通过采用的计算方法,作者谨慎地做了两个假设,这两个假设都倾向于夸大污染的计算值。因此,假设颈外动脉没有分支向脑组织供血,而且,脑外混杂物是由与颈外血液一样稀释的血液引起的。计算值为几个百分点的混杂物不会严重影响 CBF。因此可以得出结论,在一般情况下,颈内血没有发生严重的脑外污染,因此 CBF 基本上是指颅内组织,即主要是大脑。
The above mentioned conclusion from the dye injection studies of Shenkin, and Harmel and Kety is based on only eight observations in eight subjects. It cannot therefore be ruled out that gross contamination, and hence gross errors, may occur in occasional cases. Various observations have been interpreted to indicate such contamination in a small percentage of cases. Kety and Schmidt found, in 2 out of 100 studies using the original nitrous oxide method, that the venous curve failed to approach the arterial curve in the usual fashion (173). By applying the equation for CBF for each minute it became apparent that in these two cases the calculated value continued to decrease quite unusually even at the end of the experiment at 10 minutes’ inhalation of nitrous oxide. These authors recommended that such studies should be rejected as being presumably grossly contaminated.
上述来自 Shenkin 以及 Harmel 和 Kety 的染料注射研究的结论是基于 8 名受试者的 8 次观察。因此,不能排除在偶尔的情况下可能会出现严重的污染,从而出现严重的错误。各种观察结果都被解释为表明在一小部分病例中存在这种污染。Kety 和 Schmidt 发现,在 100 项使用原始氧化亚氮方法的研究中,有 2 项发现静脉曲线未能以常规方式接近动脉曲线(173)。通过应用每分钟的 CBF 方程式,可以看出在这两种情况下,即使在吸入氧化亚氮 10 分钟的实验结束时,计算出的数值仍在不寻常地减少。这些作者建议,应拒绝此类研究,因为它们可能受到严重的污染。
Scheinberg observed a marked increase in CBF in 2 out of 19 subjects to whom nicotinic acid was administered (270). The drug was found to increase the perfusion of the facial tissues, and it was concluded that in the two cases mentioned gross extracerebral contamination had caused the rise in CBF. Using the simplified, continuous sampling modification of the nitrous oxide method, Scheinberg was unable to apply the minute-to-minute calculations proposed by Kety and Schmidt (173). This is unfortunate, since such data might have revealed gross extracerebral contamination even in the control studies of the two subjects who subsequently reacted abnormally to nicotinic acid. From the data presented by Scheinberg, the possibility cannot be excluded that an increase of the cerebral perfusion rate had actually occurred in these two subjects. In order to evaluate this possibility, it would have been of importance if the arterial carbon dioxide tension and the respiratory quotient of the tissue had been reported.
Scheinberg 观察到 19 名受试者中,有 2 名受试者的 CBF 明显增加,他们被注射了烟酸(270)。发现该药物增加了面部组织的灌注,并得出结论,在上述两个病例中,脑外的严重污染导致了 CBF 的上升。使用氧化亚氮方法的简化、连续采样修改,Scheinberg 无法应用 Kety 和 Schmidt(173)提出的逐分钟计算。这是不幸的,因为这样的数据可能揭示了脑外的严重污染,甚至在后来对烟酸有异常反应的两个受试者的对照研究中也是如此。从 Scheinberg 提供的数据来看,不能排除这两个受试者的脑灌注率确实发生了增加的可能性。为了评估这种可能性,如果能报告动脉二氧化碳张力和组织的呼吸商数就会很重要。
Hyperventilation studies have been interpreted to indicate gross extracerebral contamination in 9 out of 69 determinations (75, 200). In these nine cases, hyperventilation failed to decrease the oxygen saturation of the internal jugular blood. Variations in the exact site of sampling of internal jugular blood might be implicated, in view of the fact that other investigators have not reported similar cases of non-responsiveness in any out of 33 cases (106, 171, 192). Such variations in sampling site may also explain the observations of Kety and Schmidt (173) and of Scheinberg (270) mentioned above.
过度通气研究被解释为在 69 次测定中的 9 次表明了脑外严重污染(75,200)。在这 9 个案例中,过度通气未能降低颈内静脉血的氧饱和度。鉴于其他研究者在 33 个病例中没有报告类似的无反应病例,因此可能牵涉到颈内静脉血采样的确切部位的变化(106,171,192)。采样部位的这种变化也可以解释上文提到的 Kety 和 Schmidt(173)以及 Scheinberg(270)的观察。
From the discussion in this section it may be surmised that there are reasons to believe that the blood in the internal jugular vein at its exit from the skull is derived predominantly from the intracranial tissues. Failure to puncture the vein correctly may well be the cause of gross contamination which is found occasionally. Such studies should be rejected. It would be desirable if more data were available regarding the criteria for rejecting such studies. In the experience of the author, it is usually not too difficult to recognize gross contamination, since such cases will fall quite out of line with other studies in comparable cases studied under comparable conditions. When an intermittent sampling method is employed, application of the CBF equations from minute to minute affords a valuable criterion. In addition, unusually low values for the CBF and the arteriovenous oxygen difference are found. Thus, exceedingly low CMRO2 values are found in grossly contaminated cases, while the oxygen saturation of the internal jugular vein may be unusually high. Low values for the respiratory quotient may also be found. If bilateral sampling of the internal jugular veins has been performed and only one side is grossly contaminated, then unusually large side-to-side differences of CBF and CMRO2 may be found. Perhaps a brief period of hyperventilation might constitute an additional criterion for the origin of the venous blood sampled.
从本节的讨论中可以推测出,有理由相信颈内静脉在离开颅骨时的血液主要来自颅内组织。未能正确穿刺静脉很可能是偶尔发现的严重污染的原因。这样的研究应该被拒绝。如果有更多关于拒绝这类研究的标准的数据,那就更好了。根据笔者的经验,通常不难识别严重污染,因为这种情况与其他在类似条件下研究的类似病例的研究结果很不一致。当采用间歇性采样方法时,每分钟的 CBF 方程式的应用提供了一个宝贵的标准。此外,还发现 CBF 和动静脉氧差的数值异常低。因此,在严重污染的病例中会发现超低的 CMRO2 值,而颈内静脉的氧饱和度可能异常的高。也可能发现呼吸商的低值。如果对颈内静脉进行了双侧取样,并且只有一侧被严重污染,那么可能会发现 CBF 和 CMRO2 的侧向差异异常大。也许短暂的过度通气可能构成采样的静脉血来源的一个额外标准。
It must be emphasized that gross contamination is rare, that it is usually easily recognized, and that it can possibly be kept to a minimum by using a meticulous technique in puncturing the internal jugular vein. The detailed description of the technique by Gibbs, Lennox and Gibbs (106) is very useful, and it is important to strive to place the needle as high as possible. When unusual difficulty in placing the needle is encountered or when it is felt that the final position of the needle is unusual, then, in the experience of the present author, gross contamination is more likely to occur.
必须强调的是,严重污染是罕见的,它通常很容易被识别,而且通过使用细致的技术穿刺颈内静脉,它可能被控制在最低限度。Gibbs、Lennox 和 Gibbs (106) 对该技术的详细描述非常有用,重要的是努力将针头放在尽可能高的位置。当遇到不寻常的放针困难时,或者觉得放针的最终位置不寻常时,那么根据本作者的经验,更有可能发生严重污染。
# 单侧和双侧的脑血流
Unilateral and Bilateral Cerebral Blood Flow
The calculated CBF is only representative of the whole brain if it can be assumed that the venous blood sampled is representative of mixed cerebral venous blood. It is quite likely that the bulk of the cerebral venous blood drains normally via the internal jugular veins in the human subject. Anatomical observations (117) and the rapid and marked rise in cerebrospinal fluid pressure following sudden compression of both internal jugular veins, favor this conclusion. For this reason it may be stated, without gross oversimplification, that if the blood in the two internal jugular veins always is identical, then a unilateral study gives CBF and CMRO2 values representative of the whole brain. But if different CBF and CMRO2 values occur on the two sides, then a unilateral study cannot with certainty be representative of the whole brain. In cases where significant side-to-side differences exist, a unilateral study refers only to that unknown part of the brain draining to the vein actually punctured. Sampling from both internal jugular veins simultaneously, i.e. bilateral studies, becomes in this situation the only possible method of obtaining values representative of the whole brain. Several bilateral studies have been reported (11, 61, 145, 173, 234, 271, 303). It is now established that side-to-side differences which are not due to random technical errors do occur in a high proportion of both normal subjects and subjects with various pathological conditions (234). In many cases these differences are quite small, but in some cases they are more pronounced.
只有当可以假设采样的静脉血是代表混合脑静脉血时,计算出的 CBF 才能代表整个大脑。很可能大部分的脑静脉血是通过人体的颈内静脉正常排出的。解剖学观察(117)和突然压迫两条颈内静脉后脑脊液压力的迅速和明显上升,都有利于这一结论。由于这个原因,可以说,在不严重过度简化的情况下,如果两条颈内静脉中的血液总是相同的,那么单侧研究给出的 CBF 和 CMRO2 值可以代表整个大脑。但如果两侧的 CBF 和 CMRO2 值不同,那么单侧研究就不能肯定地代表全脑的情况。在两侧存在明显差异的情况下,单侧研究仅指大脑引流至实际穿刺的静脉的未知部分。在这种情况下,从两条颈内静脉同时取样,即双侧研究,成为获得代表全脑的数值的唯一可能方法。已有一些双侧研究报告(11,61,145,173,234,271,303)。现在已经确定,在正常人和有各种病理状况的受试者中,确实有很大比例的侧向差异不是由于随机技术错误造成的(234)。在许多情况下,这些差异是相当小的,但在某些情况下,它们是比较明显的。
The standard deviation of the difference between the unilateral CBF and the bilateral value can be calculated to be about 10 per cent of CBF (234). Kety and Schmidt presented evidence to show that this source of variation was not materially greater than that due to random experimental errors of the N2O technique (173). It was concluded that “. . . in the great majority of individuals, blood from one internal jugular at the superior bulb is fairly representative of mixed cerebral venous blood. . . .” (173). Munck and Lassen found that the Kr85 method was more accurate. Therefore, using this method, the very same side-to-side differences became a major source of variation (234). It was concluded, that . bilateral values reflect the blood flow and oxygen consumption of the whole brain much more reliably than unilateral values.”
单侧 CBF 和双侧值之间差异的标准差可计算出约为 CBF 的 10%(234)。Kety 和 Schmidt 提出的证据表明,这种变化的来源并不比 N2O 技术的随机实验误差大多少(173)。结论是:"...... 在绝大多数人中,来自上球部一个颈内静脉的血液是相当代表混合脑静脉血液的。. ." (173). Munck 和 Lassen 发现 Kr85 方法更准确。因此,使用这种方法,非常的侧向差异成为变化的主要来源(234)。结论是,. 双侧值比单侧值更可靠地反映了整个大脑的血流量和耗氧量 "。
A final evaluation of the physiological significance of the side-to-side differences is not possible at present. The position of the jugular needles relative to the blood stream could be of importance if pronounced streaming was present. But then, reinserting a needle during a study would be expected occasionally to give rise to an abrupt discontinuity of the venous inert gas saturation curve. Such a phenomenon has never been observed as far as we know. It is unlikely that side-to-side differences found are caused only by varying amounts of extracerebral contamination. In the average case such contamination is, according to dye injection studies (306), presumably in the order of a few percentages, whereas the average side-to-side difference of CBF has been found to be about 15 per cent (234). It can be calculated that variations of a contamination of this magnitude alone can hardly be expected to account for the whole side-to-side variation observed.
目前还不可能对两侧差异的生理意义进行最终评估。如果存在明显的血流,那么颈部针头相对于血流的位置可能是重要的。但是,在研究过程中重新插针,预计偶尔会引起静脉惰性气体饱和度曲线的突然中断。据我们所知,这种现象从未被观察到。所发现的两侧差异不太可能只是由不同数量的脑外污染造成的。根据染料注射研究(306),在一般情况下,这种污染可能是几个百分点,而 CBF 的平均侧向差异已被发现约为 15%(234)。可以计算出,仅这种程度的污染变化就很难解释观察到的整个侧向变化。
Thus it appears likely that the side-to-side differences represent, to some extent at least, true differences between the cerebral venous blood draining via the right and left internal jugular veins. According to this explanation, the side with the higher CBF drains proportionally more venous blood from highly perfused brain tissues than the side with the lower CBF. Accepting this explanation, one further assumption is necessary in order to calculate a representative CBF value. It is necessary to know the ratio of the total blood flow of the two internal jugular veins. No information on this ratio is available. The assumption has been made that both jugulars drain the same amount of blood (234), but more complicated calculations have also been proposed (189). As the side-to-side differences are usually not excessive, moderate variations of this ratio, e.g. between 0.5 and 2.0, will not affect the result markedly.
这样看来,侧面的差异至少在某种程度上代表了通过左右颈内静脉排出的脑静脉血之间的真正差异。根据这一解释,CBF 较高的一侧比 CBF 较低的一侧从高灌注的脑组织中排出的静脉血比例更高。接受这一解释,为了计算有代表性的 CBF 值,还有一个假设是必要的。有必要知道两个颈内静脉的总血流量的比例。目前还没有关于这个比率的信息。有人假设两条颈静脉排血量相同(234),但也有人提出更复杂的计算方法(189)。由于两侧的差异通常不大,这个比例的适度变化,例如在 0.5 和 2.0 之间,不会明显影响结果。
Only few series of bilateral studies have been published so far (145, 173, 234, 271, 303). The largest series was reported by Munck and Lassen (234) using Kr85 as the inert gas, and a multiple sample technique. On the basis of their observations, it may be concluded that the bilateral approach, using an accurate technique, seems to increase the accuracy of the individual observation, to reduce the standard deviation (especially of the calculated cerebral oxygen uptake value) in homogeneous clinical groups, and to increase the coefficients of correlation. It should be emphasized, however, that no systematic side-to-side predominance has been found in normal man or in a number of clinical conditions (11, 61, 145, 173, 234, 271). Therefore, in a series of cases, the mean of unilateral measurements would be as representative of the whole brain as bilateral measurements; only the standard deviation would be greater. Almost all conclusions drawn from studies using unilateral techniques have been based on measurements of fairly large series of subjects. It appears very unlikely that any positive conclusion from such unilateral studies is in error because of side-to-side differences of CBF and CMRO2.
到目前为止,只发表了几个系列的双边研究(145, 173, 234, 271, 303)。最大的系列是由 Munck 和 Lassen(234)报告的,使用 Kr85 作为惰性气体,并采用多样品技术。根据他们的观察,可以得出这样的结论:使用准确的技术的双侧方法似乎可以提高个体观察的准确性,减少同质临床群体中的标准偏差(尤其是计算的脑摄氧量值),并提高相关系数。然而,应该强调的是,在正常人或一些临床情况下,没有发现系统性的侧向优势(11, 61, 145, 173, 234, 271)。因此,在一系列病例中,单侧测量的平均值将和双侧测量一样代表整个大脑;只是标准差会更大。从使用单侧技术的研究中得出的几乎所有结论都是基于对相当大系列受试者的测量。由于 CBF 和 CMRO2 的侧向差异,从这种单侧研究中得出的任何积极结论似乎都不可能是错误的。
Systematic side-to-side differences have been found only in some cases of intracranial arteriovenous aneurysms (26, 28, 33, 189, 286, 312) and immediately following surgical obliteration of one carotid artery in one elderly subject (303). In diffuse chronic cerebral disease, findings suggestive of a consistent difference of the cerebral oxygen uptake values of the right and left internal jugular have recently been obtained in a bilateral study by Lassen, Lane and Feinberg (unpublished observations). Studying a series of aged mental hospital patients with signs suggestive of organic brain damage, it was found that the bilateral and the left side values for cerebral oxygen uptake correlated much more closely than the corresponding right side values to the degree of mental deterioration assessed from clinical data and psychological test results. This finding may be interpreted to indicate that disease of the left side of the brain is of more direct importance for the development of mental deterioration than a comparable right-sided cerebral process. As mentioned, no previous study has shown a consistent side-to-side predominance. It seems that further experimental evidence is necessary in order to determine whether or not left-sided unilateral values do actually show a closer agreement with mental function than the corresponding right-sided values.
只有在一些颅内动静脉瘤的病例中(26,28,33,189,286,312),以及在一位老人的颈动脉手术切除后(303),才发现系统性的两侧差异。在弥漫性慢性脑病中,最近 Lassen、Lane 和 Feinberg(未发表的意见)在一项双侧研究中获得了暗示左右颈内动脉的脑氧摄取值有一致差异的结果。研究了一系列具有提示有机脑损伤迹象的老年精神病院病人,发现双侧和左侧的脑氧摄取值与根据临床数据和心理测试结果评估的精神恶化程度的相关性比相应的右侧值要密切得多。这一发现可被解释为表明,与可比的右侧大脑过程相比,左侧大脑的疾病对精神恶化的发展具有更直接的重要性。如前所述,以前的研究没有显示出一致的侧向优势。看来需要进一步的实验证据,以确定左侧单侧的数值是否确实比相应的右侧数值与精神功能更接近。
# 其他评论
Additional Comments
By the very nature of the method, the CBF refers to all tissues exchanging inert gas with blood subsequently draining via the superior bulb of the internal jugular. For this reason the unit of reference, Too gm brain’, must be thought of as 100 grams of all tissues taken approximately in their actual proportion by weight.
根据该方法的性质,CBF 指的是所有组织与血液交换惰性气体,然后通过颈内静脉的上球体排出。由于这个原因,参考单位 "Too gm brain" 必须被认为是 100 克的所有组织按其实际重量比例取值。
Non-cerebral tissues, exchanging inert gases and/or oxygen and contributing to the venous blood sampled, do not necessarily have the same partition coefficient as the brain. This means that tissues such as the cerebrospinal fluid (188) and the orbital fat (191) are represented in Too gm brain’ in proportion to the ratio of their weight and their relative inert gas solubility (the tissue inert gas solubility is, in this connection, taken relative to that of the whole brain). Furthermore, if any of the contributing tissues have a very slow clearance rate of inert gas, then they will be represented less in the Too gm brain’ than in proportion to their weight. When extrapolating to infinity, it is likely that all cerebral tissues— even slowly perfused areas such as the white matter of the brain—are adequately taken into account. (See the discussion in the section on the effect of heterogeneous cerebral perfusion.) Very slow inert gas uptake, however, is likely to occur in non-cerebral tissues such as the liquor cerebrospinalis (6, 32, 199), the meninges, the orbital adipose tissue, and part of any contribution from the facial tissues. The supposedly already small contribution of such tissues to the calculated cerebral blood flow is thus further minimized.
非脑组织,交换惰性气体和 / 或氧气并对静脉血采样有贡献,不一定具有与脑相同的分配系数。这意味着诸如脑脊液(188)和眼眶脂肪(191)等组织在 "Too gm brain" 中的比例与它们的重量和相对惰性气体溶解度(在这方面,组织的惰性气体溶解度是相对于整个大脑的惰性气体溶解度而言的)。此外,如果任何一个组织对惰性气体的清除率很慢,那么它们在 "Too gm 脑" 中的比例就会比它们的重量要低。当推算到无穷大时,很可能所有的脑组织 -- 甚至像脑白质这样的缓慢灌注区域 -- 都被充分考虑到了。(见关于异质脑灌注的影响一节中的讨论)。然而,非常缓慢的惰性气体吸收可能发生在非脑组织中,如脑脊液(6,32,199)、脑膜、眼眶脂肪组织,以及面部组织的部分贡献。因此,这些组织对计算出的脑血流的贡献应该已经很小了。
Thus the unit, Too gm brain,’ includes the cerebral tissue proper, the blood in the cerebral vessels (159), the liquor (6, 32, 199), and presumably also part of the meninges and the orbital contents. A correction for the blood content of the cerebral vessels has been attempted by Lassen and Munck (188). The correlation was based on crude estimates of the mean circulation time over the brain, and is of doubtful value. Variations of the intracranial blood volume do apparently occur (260, 308, 346), but are presumably too small to be of any real importance. Undoubtedly the CBF reflects predominantly the perfusion of the hemispheres, as they form the bulk of the brain.
因此,"Too gm brain" 这个单位包括脑组织本身、脑血管中的血液(159)、液体(6、32、199),以及可能还有部分脑膜和眼眶内容物。Lassen 和 Munck(188)曾尝试对脑血管中的血液含量进行校正。这种关联是基于对大脑平均循环时间的粗略估计,其价值值得怀疑。颅内血量的变化显然是有的(260,308,346),但估计太小,没有任何实际意义。毫无疑问,CBF 主要反映的是半球的灌注情况,因为它们构成了大脑的主体。
As the unit of reference is 100 gm. of perfused tissue, the CBF is not influenced by the absolute size of the brain or by localized complete infarction of the brain. This aspect of the method is of some importance for evaluating the results obtained in clinical conditions such as microcephaly (78) or acute cerebrovascular accidents (199). In many conditions it may be considered an advantage, however, that the results do not reflect individual variations in brain weight.
由于参考单位是 100 克的灌注组织,CBF 不受大脑绝对大小或大脑局部完全梗塞的影响。该方法的这一方面对于评估在小脑症(78)或急性脑血管意外(199)等临床情况下获得的结果具有一定的重要性。然而,在许多情况下,可以认为是一种优势,因为其结果不反映大脑重量的个体差异。
The accuracy of the inert gas method has never been established in man, as no suitable independent method without error is available. Kety and Schmidt’s monkey studies did, however, demonstrate that the error of the method is likely to be quite small (173). The influence of side-to-side variations has been discussed, and it was pointed out that the difference between a unilateral CBF and the corresponding value has a standard deviation of about 10 per cent of CBF. Random errors of a technical nature also influence the measurements. The magnitude of these errors and of biological variants with time has been determined by analyzing the results obtained in series of paired unilateral studies repeated on the same individual and under the same experimental conditions within a time interval of about 30 minutes. Regarding unilateral CMRO2, a standard deviation of 0.19 cc per loogm per minute, or about 6 per cent of the average CMRO2, was found using the original N2O method (173). Using Scheinberg and Stead’s modification of the N2O method, a greater random error of unilateral values must be expected. This modification also gives systematically higher values than the original method (173, 284), presumably due to timing and dilution errors (333). The Kr86 technique appears to be the most accurate modification thus far developed. The variation of unilateral CMRO2 calculated from repeated unilateral studies was 0.13 cc per loogm per minute (188). This variation is about 4 per cent of the average CMRO2 of the cases studied. Theoretical (234) and experimental (188) attempts have been made to determine more rigorously the effect of random analytical errors on unilateral CBF and CMRO2. As it is possible that these approaches did not include all random errors, the error estimates arrived at will not be discussed further. No experimental evidence is available for the evaluation of the accuracy of the direct method of measuring total cerebral blood flow using y-emitting inert gases (197, 198). Presumably the continuous measurement of the amount of radioactivity in the brain alone—excluding all other sources of radiation—is subject to quite a considerable error.
惰性气体法的准确性从未在人身上得到证实,因为没有合适的无误差的独立方法可用。然而,Kety 和 Schmidt 的猴子研究确实证明了该方法的误差可能相当小(173)。已经讨论了侧向变化的影响,并指出单侧 CBF 与相应值之间的差异,其标准偏差约为 CBF 的 10%。技术性的随机误差也会影响测量结果。这些误差的大小以及随时间变化的生物变异已经通过分析在同一人身上和相同的实验条件下,在大约 30 分钟的时间间隔内重复进行的一系列成对单侧研究的结果来确定。关于单侧 CMRO2,使用原始的 N2O 方法发现标准偏差为每分钟 0.19 毫升,或平均 CMRO2 的大约 6%(173)。使用 Scheinberg 和 Stead 对 N2O 方法的修改,必须预期单侧数值的随机误差更大。这种修改也给出了比原始方法更系统的数值(173,284),可能是由于时间和稀释误差(333)。Kr86 技术似乎是迄今为止开发的最准确的修改方法。从重复的单侧研究中计算出的单侧 CMRO2 的变化是每分钟 0.13cc/loogm(188)。这一变化约为所研究病例的平均 CMRO2 的 4%。理论上(234)和实验上(188)都试图更严格地确定随机分析误差对单侧 CBF 和 CMRO2 的影响。由于这些方法可能没有包括所有的随机误差,所得出的误差估计值将不会进一步讨论。没有实验证据可用于评估使用 y 发射的惰性气体直接测量总脑血流的准确性(197,198)。据推测,仅对大脑中的放射性量进行连续测量 -- 不包括所有其他辐射源 -- 就会出现相当大的误差。
# 指示剂注射法
Indicator Injection Method
Gibbs, Maxwell and Gibbs (no) have applied the Stewart-Hamilton techniques (132, 133, 326-330) to the study of cerebral circulation in man. A known amount of a biologically inert indicator, such as Evans blue dye (T-1824), is injected into one of the internal carotid arteries, and the dilution of indicator is followed by sampling from one or both internal jugular veins. By this method the total cerebral blood flow can be calculated. By simultaneously determining the arteriovenous difference of oxygen or other metabolites the metabolic rate of the whole brain of such compounds can also be calculated2. A continuous injection of indicator over a period of at least 2 minutes was employed in the original method of Gibbs, Maxwell and Gibbs (no). Instantaneous injection was employed by another group, a modification which reduced the duration of the experiment to less than 1 minute (306). Mylin and Bldmer have further modified the method by using multiple venous samples instead of integrated samples (242, 243). Thus it became possible to calculate in addition the cerebral mean circulation time and vascular volume of the brain. The method is based on several assumptions, some of which have already been discussed in connection with the inert gas diffusion method. Thus it is superfluous to repeat the arguments in favor of the conclusion that the internal jugulars carry the bulk of the cerebral venous blood without significant extracerebral contamination. Also, the assumption of constancy of total cerebral blood flow during an experiment lasting a few minutes, or even less, would seem to be valid in the majority of conditions. Undoubtedly the requirement of physiological inertness is adequately fulfilled when using small amounts of T-1824 or thorium B-labeled red cells (242, 243) as the indicator. Moreover, these indicators can be assumed not to be retained or metabolized in the brain. The injection of a known amount of indicator into an internal carotid artery poses a major technical problem. Most investigators have used percutaneous carotid puncture, and presumably errors of injection may occur occasionally.
Gibbs、Maxwell 和 Gibbs(没有)将 Stewart-Hamilton 技术(132, 133, 326-330)用于研究人的脑循环。将已知量的生物惰性指标,如埃文斯蓝染料(T-1824),注入其中一条颈内动脉,然后从一条或两条颈内静脉取样稀释指标。通过这种方法可以计算出总的脑血流量。通过同时测定氧气或其他代谢物的动静脉差异,也可以计算出这种化合物的全脑代谢率 [2](#bookmark5)。在 Gibbs, Maxwell 和 Gibbs (no) 的原始方法中,采用了在至少 2 分钟的时间内连续注入指示剂的方式。另一个小组采用了瞬时注射法,这一修改将实验时间减少到 1 分钟以内(306)。Mylin 和 Bldmer 进一步修改了该方法,用多个静脉样本代替综合样本(242,243)。这样就有可能另外计算出大脑的平均循环时间和大脑的血管容积。该方法基于几个假设,其中一些已经在惰性气体扩散法中讨论过了。因此,重复支持以下结论的论据是多余的,即颈内静脉携带大部分脑静脉血,没有明显的脑外污染。另外,在一个持续几分钟甚至更短的实验中,脑血流总量不变的假设似乎在大多数情况下都是有效的。毫无疑问,当使用少量的 T-1824 或钍 B 标记的红细胞(242,243)作为指标时,生理惰性的要求得到了充分的满足。此外,可以假定这些指示剂不会在大脑中被保留或代谢掉。将已知数量的指示剂注入颈内动脉是一个主要的技术问题。大多数研究者都使用经皮颈动脉穿刺,据推测,注射错误可能偶尔会发生。
The problem of recirculation of indicator is not very great, due to the large dilution in the central blood volume. This error can be reduced by subtracting the recirculating arterial indicator concentration from the cerebral venous concentration (no, 306). The use of highly diffusible indicators would reduce recirculation, but would also increase the time needed for washout from the brain. Radioactive potassium might offer some advantage, as it remains largely intravascular during the first transit through the brain but leaves the blood stream rapidly in other tissues (47, 268).
由于中心血量的大量稀释,指标再循环的问题不是很大。通过从脑静脉浓度中减去再循环的动脉指示剂浓度,可以减少这种误差(不,306)。使用高扩散性指标会减少再循环,但也会增加从大脑中洗出的时间。放射性钾可能会提供一些优势,因为它在第一次通过大脑的过程中基本上保持在血管内,但在其他组织中则迅速离开血流(47,268)。
The indicator is usually injected into only one of the internal carotid arteries. Thus it is not surprising that pronounced side-to-side differences often occur between the indicator dilution curves of the two internal jugular veins (242-244, 306). The side-to-side differences are of much greater magnitude than those observed with the inert gas method, in which the gas reaches the brain in the same concentration via all arteries. The side-to-side differences of injected indicator are also very variable. Usually the ipsilateral jugular has a higher concentration than the contralateral, but in some instances the opposite is found. This means that unilateral measurements cannot be assumed to be representative of the whole brain (155). Only if the opposite jugular is occluded can a unilateral study be reasonably accurate. It is uncertain, however, whether in this situation the bulk of the cerebral venous blood actually drains via the patent jugular. Compression of the contralateral jugular was used by Gibbs, Maxwell and Gibbs in an isolated study. In this case the total outflow of one internal jugular measured directly compared favorably to the results obtained by the indicator injection method (no). This unique experiment is the only case in which a direct measurement of the cerebral blood flow in man has been attempted. Bilateral studies seem to offer a more reliable approach to avoid the influence of side-to-side differences without disturbing the venous outflow. The magnitude of these differences implies, however, that variations in the ratio of total flow of the two jugulars have a greater influence on the accuracy of the results than when using the inert gas method.
指示剂通常只注射到颈内动脉中的一条。因此,两个颈内静脉的指示剂稀释曲线之间经常出现明显的侧向差异也就不奇怪了(242-244,306)。侧面的差异比惰性气体法观察到的要大得多,在惰性气体法中,气体通过所有动脉到达大脑的浓度相同。注射指标的侧向差异也是非常可变的。通常同侧颈部的浓度高于对侧,但在某些情况下,情况正好相反。这意味着不能认为单侧的测量结果就能代表整个大脑(155)。只有当对侧颈动脉闭塞时,单侧的研究才会有合理的准确性。但不确定的是,在这种情况下,大部分的脑静脉血是否真的通过通畅的颈静脉排出。Gibbs、Maxwell 和 Gibbs 在一项单独的研究中使用了压迫对侧颈静脉的方法。在这种情况下,直接测量的一个颈内静脉的总流出量与指标注射法得到的结果相比是很好的(没有)。这个独特的实验是唯一尝试直接测量人的脑血流的案例。双侧研究似乎提供了一个更可靠的方法,以避免侧向差异的影响而不干扰静脉的流出。然而,这些差异的大小意味着,与使用惰性气体法相比,两个颈部总流量比例的变化对结果的准确性影响更大。
The indicator injection method has so far only been used in a single clinical study (104). In the following discussion, when reference is made to studies of cerebral blood flow and metabolism, the inert gas method has been used unless otherwise stated. It is to be hoped, however, that bilateral studies using the indicator injection method will be employed more extensively in the future. In many clinical studies, such as degenerative cerebral diseases, it would be of interest to study the total flow and oxygen uptake of the brain. These values cannot be obtained by the inert gas method unless the modification using 7-emitting isotopes is employed, a modification which is technically quite involved and presumably less accurate. Unilateral or bilateral studies employing the injection of several indicators simultaneously seem to be a promising approach for the study of the transcapillary exchange of a variety of compounds. Thus far such dynamic studies of the blood-brain barrier have been made only in a small number of animal experiments by Chinard and associates (47).
到目前为止,指标注射法只在一项临床研究中使用过(104)。在下面的讨论中,当提到脑血流和新陈代谢的研究时,除非另有说明,否则都是使用惰性气体法。不过,希望今后能更广泛地采用指标注射法进行双边研究。在许多临床研究中,如退行性脑病,研究大脑的总流量和氧摄取量将是有意义的。这些数值不能通过惰性气体法获得,除非采用使用 7 - 发射同位素的修改方法,这种修改方法在技术上相当复杂,而且可能不太准确。单侧或双侧研究,同时注入几个指标,似乎是研究各种化合物经毛细血管交换的一个有希望的方法。到目前为止,只有 Chinard 和他的同事在少量的动物实验中对血脑屏障进行了这种动态研究(47)。
# 脑血流的调节
Regulation of Cerebral Blood Flow
In healthy young adults studied in the supine position, the cerebral blood flow is about 50-55 cc per loogm per minute, or approximately 750 cc per minute for a brain of average weight (173). Thus, the brain receives about 15 per cent of the total cardiac output of a resting subject. The cerebral perfusion is controlled very efficiently by homeostatic regulation of the perfusion pressure and the so called cerebral vascular resistance.
在仰卧位研究的健康年轻成人中,脑血流量约为每分钟 50-55 毫升,或平均重量的大脑约为每分钟 750 毫升(173)。因此,大脑接受了静止状态下总心输出量的 15% 左右。通过对灌注压力和所谓的脑血管阻力的稳态调节,脑灌注得到了非常有效的控制。
# 大脑的灌注压力
Perfusion Pressure of the Brain
The pressure difference between the cerebral arteries and veins is the driving force of the cerebral circulation. The pressure in the cerebral veins is usually only a few mm Hg above the atmospheric pressure. For this reason the arterial blood pressure at the level of the head will in most situations adequately represent the cerebral perfusion pressure. Only in positive gravitational stress is the cerebral venous pressure the decisive factor in maintaining an adequate pressure differece. Studies during acute acceleration to 4-5 g have shown that the arterial pressure at brain level is reduced to a few mm Hg, while simultaneously the pressure in the cranial part of the internal jugular veins drops to as low as —60 mm Hg (136). In the erect posture, and on exposure to normal gravitational forces, the driving pressure of the human brain is only slightly reduced. This very moderate pressure decrease can hardly be the cause of the reported reduction of cerebral blood flow to about 80 per cent of the values in the supine position (247, 252, 284, 310). This reduction most likely results from a decrease in the arterial pCO2 (147). The effect of a primary increase of the jugular pressure to a moderately elevated level of 235 mm H2O was studied by Moyer and associates (225). The cerebral blood flow was not significantly influenced by the pressure rise.
大脑动脉和静脉之间的压力差是大脑循环的动力。大脑静脉中的压力通常只比大气压力高几毫米汞柱。由于这个原因,在大多数情况下,头部水平的动脉血压将充分代表脑灌注压力。只有在正的重力压力下,脑静脉压力才是维持足够压力差的决定性因素。在急性加速到 4-5g 时的研究表明,脑水平的动脉压力降低到几毫米汞柱,同时颈内静脉的颅内部分的压力下降到低至 - 60 毫米汞柱(136)。在直立的姿势下,暴露在正常的重力作用下,人脑的驱动压力只是稍微降低。这种非常适度的压力下降很难成为报道的脑血流量减少到仰卧位数值的 80% 左右的原因(247, 252, 284, 310)。这种减少很可能是由于动脉 pCO2 的减少(147)。Moyer 和同事研究了将颈部压力一次提高到 235 毫米水的中等水平的效果(225)。大脑血流没有受到压力上升的明显影响。
The prime importance of the arterial blood pressure for sustaining cerebral circulation was well recognized by early investigators. Until quite recently it was generally believed that this factor alone determined the cerebral blood flow, i.e. that the cerebral vessels did not possess any significant capacity for intrinsic control of the vascular tone, so that the perfusion passively followed changes of the arterial blood pressure (141, 348). Maintenance of a relatively constant cerebral blood flow was thought to be solely the result of the homeostatic regulation of the arterial blood pressure. The location of the pressure-sensitive zones in the cranial part of the arterial tree (10) could be taken to support this concept. Recent quantitative studies in man, however, have demonstrated that—within a wide pressure range—the cerebral blood flow is independent of changes of the arterial blood pressure (fig. 1). A moderate reduction of blood pressure does not influence cerebral blood flow (58, 124-126, 206). Only in marked hypotension with pressures of half the normal value or less is cerebral vasodilatation inadequate, the cerebral blood flow falling to a critically low value of about 60 per cent of the control level, and clinical signs of cerebral hypoxia becoming apparent (81). Hypotension induced by tilting (81) or spinal anesthesia (168, 184, 185) has the same effect as a similar degree of hypotension induced by various antihypertensive drugs (24, 29, 31, 223, 224, 229, 230). Also, in hypertension cerebral blood flow remains fairly normal irrespective of the cause of the pressure rise (cf. essential hypertension, refs. 122, 131, 166, 172, 228, 229; hypertensive toxemia of pregnancy, refs. 203-212; vasopressin infusion, ref. 323; and Z-norepinephrine infusion, refs. 177, 230, 298). It may be pointed out, however, that in these various hypertensive states the possibility cannot be excluded that the cerebral vasoconstriction noted might be secondary to circulating vasoconstrictor substances. For this reason, the relative constancy of CBF in hypertension cannot be taken as definite proof of intrinsic autoregulation of cerebral vascular tone in this condition.
动脉血压对维持脑循环的首要重要性已被早期的研究者们充分认识。直到最近,人们普遍认为这个因素单独决定了脑血流,也就是说,脑血管不具备任何内在控制血管张力的重要能力,因此,灌注被动地跟随动脉血压的变化(141,348)。维持相对稳定的脑血流被认为完全是动脉血压平衡调节的结果。动脉树颅骨部分的压力敏感区的位置(10)可以被用来支持这一概念。然而,最近对人的定量研究表明,在很宽的压力范围内,脑血流与动脉血压的变化无关(图 1)。适度降低血压并不影响脑血流(58, 124-126, 206)。只有在压力为正常值一半或更低的明显低血压情况下,脑血管扩张不足,脑血流量下降到约为控制水平的 60% 的极低值,脑缺氧的临床症状才会显现(81)。倾斜(81)或脊髓麻醉(168,184,185)引起的低血压与各种抗高血压药物引起的类似程度的低血压有相同的效果(24,29,31,223,224,229,230)。另外,在高血压中,无论压力升高的原因是什么,脑血流仍然相当正常(参见基本高血压,参考文献。122, 131, 166, 172, 228, 229;妊娠高血压毒血症,参考文献。203-212;血管加压素输注,参考文献。323;和 Z - 去甲肾上腺素输注,参考文献。177, 230, 298). 然而,可以指出的是,在这些不同的高血压状态下,不能排除注意到的脑血管收缩可能是继发于循环中的血管收缩物质的可能性。由于这个原因,高血压中 CBF 的相对恒定不能作为这种情况下脑血管张力内在自动调节的明确证据。
The above mentioned clinical studies are thus in agreement with the earlier observations in animals by Fog (82-85), and by Forbes and associates (92), demonstrating that when the systemic blood pressure increased, the pial arterioles contracted; when the pressure decreased, the vessels dilated. Fog also found that the reactions of the pial arteries were qualitatively and quantitatively independent of the method used for producing the blood pressure variations (82, 85). In addition, it was demonstrated that the vascular reactivity to pressure changes was unaffected by sectioning the vagus, cervical sympathetic, sinus and aortic nerves. Subsequent studies showed that the pial arteries are fairly insensitive to the local application of sympathicomimetic drugs in doses insufficient to elevate the systemic blood pressure (84, 202). On the basis of these studies, Fog concluded that the active regulation of the cerebrovascular tone in face of variations of the blood pressure was a kind of autoregulation, possibly due to a direct effect of the pressure changes on the inherent smooth muscle tone; i.e., contraction being an automatic response of the arteries to an increase of the distending pressure and vice versa. The general principle of such a direct or so called mechanical control of the myogenic tonus of the arteries was first proposed by Biedl and Reiner (35) and by Bayliss (16, 17), and is supported by many experimental observations (see 86-88).
因此,上述临床研究与 Fog (82-85) 和 Forbes 及同事 (92) 早期在动物身上的观察结果一致,证明当全身血压升高时,皮层动脉血管收缩;当压力降低时,血管扩张。Fog 还发现,小动脉的反应在质量上和数量上都独立于血压。用于产生血压变化的方法(82,85)。此外,研究表明,切断迷走神经、颈部交感神经、静脉窦和主动脉神经,对压力变化的血管反应性不受影响。随后的研究显示,小动脉对局部应用不足以升高全身血压的拟交感神经药物相当不敏感(84,202)。在这些研究的基础上,福格得出结论,面对血压的变化,脑血管张力的主动调节是一种自动调节,可能是由于压力变化对固有平滑肌张力的直接影响;也就是说,收缩是动脉对膨胀压力增加的自动反应,反之亦然。Biedl 和 Reiner(35)以及 Bayliss(16,17)首次提出了这种直接或所谓的机械控制动脉肌张力的一般原则,并得到了许多实验观察的支持(见 86-88)。
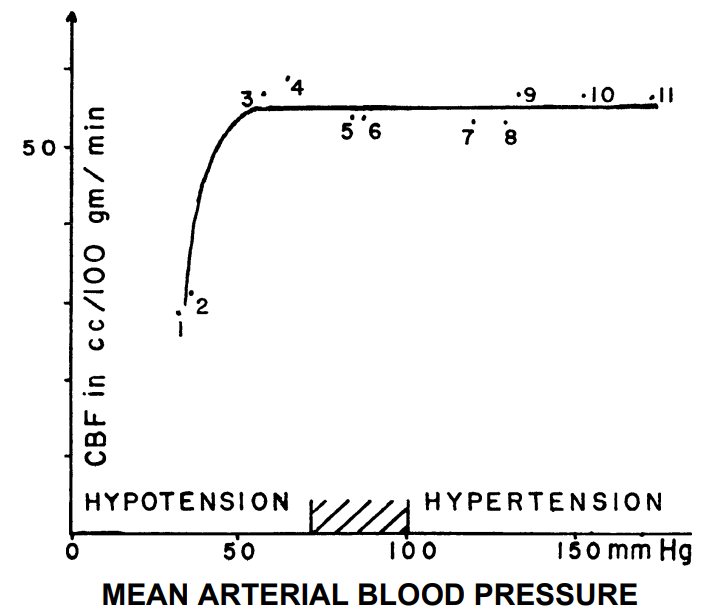
FIG. 1. Cerebral blood flow and blood pressure. Mean values of 11 groups of subjects reported in 7 studies have been plotted. Various acute and chronic conditions have been selected, characterized by a change in blood pressure. In all, this figure is based on 376 individual determinations.
1 and 2, Drug-induced severe hypotension (81). 3 and 4, Drug-induced moderate hypotension (206). 5 and 6, Normal pregnant women and normal young men (206, 173). 7, Drug-induced hypertension (230). 8, Hypertensive toxemic pregnancy (206). 9, 10,11, Essential hypertension (229, 131, 228).
图 1. 大脑血流和血压。绘制了 7 项研究中报告的 11 组受试者的平均值。选择了以血压变化为特征的各种急性和慢性情况。总的来说,该图是基于 376 个个体绘制的。
1 和 2,药物引起的严重低血压(81)。3 和 4,药物引起的中度低血压(206)。5 和 6,正常孕妇和正常青年男子(206,173)。7, 药物引起的高血压(230)。8, 妊娠毒血症引起的高血压(206)。9,10,11,基本高血压(229,131,228)。
Adjustment of local cerebral blood flow following cerebrovascular occlusion seems to be, on the local level, a situation similar to that of maintaining total cerebral blood flow in hypotension. In a recent study by Meyer and Denny-Brown, the effect of occlusion of the pial arteries was studied in monkeys by means of a variety of experimental techniques (220). Chemical factors were considered to be of minor importance for the local vasodilatation observed, since this dilatation occurred in a far wider area than that rendered hypoxic by the arterial occlusion. The authors concluded that the collateral vasodilatation was predomi-
脑血管闭塞后局部脑血流的调整,从局部来看,似乎与低血压时维持总脑血流的情况相似。在 Meyer 和 Denny-Brown 最近的一项研究中,通过各种实验技术研究了猴子的皮层动脉闭塞的影响(220)。化学因素被认为对观察到的局部血管扩张并不重要,因为这种扩张发生在比动脉闭塞所造成的缺氧更广泛的区域。作者的结论是,侧枝血管的扩张主要是由于动脉闭塞所描述的机制。
nantly due to the mechanism described by Fog, i.e., it was caused by the reduction in the local intraarterial pressure distal to the occlusion. These observations are of importance, as they seem to permit the described separate evaluation of the effect of chemical and mechanical regulatory factors on cerebral vascular tone. They form a substantial support for the theory of the existence of a mechanical control of the above mentioned type. This is noteworthy, since the many data on the intact human organism do not permit exclusion of the possibility that the autoregulation of CBF in response to blood pressure variations could be explained by chemical control of the type described in the following section.
主要是由于 Fog 所描述的机制,也就是说,它是由闭塞远端的局部动脉内压降低引起的。这些观察结果很重要,因为它们似乎允许对化学和机械调节因素对脑血管张力的影响进行描述的单独评估。它们构成了对上述类型的机械控制存在的理论的实质性支持。这是值得注意的,因为关于完整的人类机体的许多数据不允许排除这样的可能性,即 CBF 对血压变化的自动调节可以用下节所述的化学控制来解释。
Studies in man have showed that CBF is completely normal in mild hypotension as well as in essential hypertension without encephalopathy. The cerebral oxygen uptake is also normal in both conditions. The cerebral perfusion is apparently regulated in such a way as to maintain scrupulously the normal chemical milieu of the brain. This observation suggests the influence of a regulatory mechanism governed by the metabolic demands of the cerebral tissues, i.e., chemical control. It is more difficult to imagine that a local mechanical regulation from the wall of the vessels could permit the perfusion to remain so completely adequate relative to the metabolic demands. For this reason it seems likely that both mechanical and chemical factors are of importance for the autoregulation of CBF, the latter factor, however, having the final regulatory effect.
对人的研究表明,在轻度低血压以及无脑病的原发性高血压中,CBF 完全正常。在这两种情况下,脑氧摄取量也是正常的。大脑灌注的调节方式显然是为了严格维持大脑的正常化学环境。这一观察表明,由脑组织的代谢需求所支配的调节机制的影响,即化学控制。更难想象的是,来自血管壁的局部机械调节能使灌注量相对于代谢需求保持完全充足。由于这个原因,机械和化学因素对 CBF 的自动调节似乎都很重要,然而,后一个因素具有最终的调节作用。
# 大脑血管阻力
Cerebral Vascular Resistance
At any level of perfusion pressure the cerebral blood flow depends solely on the interplay of this systemic force and local impeding factors. These impeding factors form collectively the cerebrovascular resistance, which is defined as the ratio of perfusion pressure to the cerebral blood flow. (It should be pointed out that this ratio does not imply a linear relationship between pressure and flow and it is not a constant for any given subject.) The cerebrovascular resistance depends on the viscosity of the blood and on the nature of the intracranial vascular bed.
在任何水平的灌注压下,脑血流完全取决于这种系统性力量和局部阻碍因素的相互作用。这些阻碍因素共同构成了脑血管阻力,它被定义为灌注压与脑血流的比率。(应该指出的是,这个比率并不意味着压力和流量之间的线性关系,它对任何特定的对象来说都不是一个常数)。脑血管阻力取决于血液的粘度和颅内血管床的性质。
Significant changes in the viscosity of the blood are achieved by fairly marked alterations in the erythrocyte concentration or the temperature of the blood. In severe anemia a marked decrease in cerebrovascular resistance is observed (137, 261, 275), whereas in polycythemia (238, 292) and hypothermia (181) it is increased. There is no doubt that changes in physical viscosity must play a role in these conditions. It is quite possible, however, that chemical control of the diameter of the cerebral vascular bed is of decisive importance, since in all three conditions the cerebral perfusion is adjusted quite accurately to the metabolic requirements of the brain as judged from the normal level of the oxygen and carbon dioxide tensions of the cerebral venous blood.
血液粘度的明显变化是通过红细胞浓度或血液温度的相当明显的改变实现的。在严重贫血的情况下,脑血管阻力明显下降(137,261,275),而在多血症(238,292)和低温症(181)中,脑血管阻力会增加。毫无疑问,在这些情况下,物理粘度的变化一定会起到作用。然而,很有可能的是,对脑血管床直径的化学控制具有决定性的意义,因为在所有这三种情况下,脑灌注是根据脑静脉血氧和二氧化碳张力的正常水平来判断的,非常准确地调整脑的代谢要求。
The nature of the intracranial vascular bed is of major importance to cerebrovascular resistance. In this respect it is convenient to discuss three aspects of this vascular bed separately: /) the vascularity of the intracranial tissues, 2) the passive changes of vascular diameter due to changes of the intracranial pressure, and 5) the active changes of the diameter and/or tone of the vessels due to changes of the vasomotor activity of the smooth muscle cells of the vessel walls.
颅内血管床的性质对脑血管阻力具有重要意义。在这方面,分别讨论该血管床的三个方面是很方便的。/ 颅内组织的血管性,*2)* 由于颅内压力的变化引起的血管直径的被动变化,以及 5) 由于血管壁平滑肌细胞的血管运动活动的变化引起的血管直径和 / 或张力的主动变化。
Intracranial vascularity may be taken to embrace all morphological or anatomical features of the intracranial vascular bed. Thus it comprises the number of vessels, their diameter, their length, and their mutual interconnection. In intracranial arteriovenous aneurysms the cerebrovascular resistance is markedly decreased because of an abnormally increased intracranial vascularity (312). In chronic degenerative cerebral diseases the cerebral vascular resistance is increased (96). Decreased vascularity of the brain is presumably implicated, reducing the number of vessels as well as their size, a process in which arteriosclerotic vascular disease may or may not play a role.
颅内血管可被视为包括颅内血管床的所有形态或解剖特征。因此,它包括血管的数量、直径、长度以及它们之间的相互联系。在颅内动静脉瘤中,由于颅内血管的异常增加,脑血管阻力明显下降(312)。在慢性退行性脑部疾病中,脑血管阻力增加(96)。大脑血管的减少可能与此有关,减少了血管的数量以及它们的大小,这个过程中,动脉硬化性血管疾病可能起作用,也可能不起作用。
Intracranial pressure is presumably nearly the same in all conditions as the pressure in the thin-walled pial veins. Thus, even marked variations in absolute pressure in the veins, e.g. those produced by changes of posture, result in little change in the actual distending pressure of these vessels. By this mechanism the cerebral veins and capillaries are protected against collapse as well as against extreme distention. Hence the variations in intracranial pressure constitute a highly efficient ‘permanent anti-^-suit’ for the brain. In the resting recumbent position, the intracranial pressure usually varies only moderately. These variations parallel variations in cerebral blood flow, presumably because increased flow tends to cause an increased pressure in the cerebral vessels and an increased intracranial blood content, and vice versa (260, 304, 308, 346). The intracranial pressure is presumably also of importance for the circulation in the cerebral arteries. The intracranial pressure may be taken to reflect the external pressure upon the walls of the cerebral arteries, and it is thus the one of the two pressures which determine the distending pressure of the arteries. This means that with regard to the influence on the cerebral arteries an increase of intracranial pressure equals a decrease of arterial blood pressure, and vice versa. In accordance with the previous discussion, it follows that mechanical and chemical factors may both be of importance for the dilatation of the pial arteries which follows an increase of intracranial pressure (82). Changes of posture induce variation of the intracranial pressure, but also cause similar variations in the intra-arterial pressure. Hence the distending pressure of the arteries remains essentially unchanged, just as is the case with the distending pressure of the veins. A primary rise in the intracranial pressure constricts the outflow from the cerebral venous channels. At the same time the increased pressure tends to cause arterial vasodilatation, as just mentioned. However, if a rise in arterial blood pressure occurs this latter effect is presumably counteracted. The net effect of a moderate induced rise of intracranial pressure on cerebrovascular resistance is probably small. No experimental studies of the effect of a primary rise of the intracranial pressure on CBF and CMRO2 have been reported. Indirect evidence, however, suggests that the cerebral circulation remains adequate when the intracranial pressure is increased for 5-10 minutes to about 500 mm H2O (349). The cerebral circulation of patients with increased intracranial pressure associated with brain tumor will be discussed later in this review.
颅内压在任何情况下都可能与薄壁静脉中的压力几乎相同。因此,即使静脉中的绝对压力有明显的变化,例如那些由姿势变化产生的变化,也会导致这些血管的实际膨胀压力变化很小。通过这种机制,脑静脉和毛细血管得到了保护,既能防止塌陷,又能防止极端膨胀。因此,颅内压的变化对大脑来说构成了一种高效的 "永久防 ^ 服"。在静止的卧位上,颅内压通常只有适度的变化。这些变化与脑血流的变化平行,大概是因为血流的增加往往会导致脑血管内压力的增加和颅内血液含量的增加,反之亦然(260, 304, 308, 346)。颅内压可能对脑动脉的循环也有重要意义。颅内压可以被认为是反映了脑动脉壁上的外部压力,因此它是决定动脉膨胀压力的两个压力之一。这意味着就对脑动脉的影响而言,颅内压的升高等于动脉血压的降低,反之亦然。根据前面的讨论,机械和化学因素对颅内压升高后的脑动脉扩张可能都很重要(82)。姿势的改变会引起颅内压的变化,但也会引起动脉内压的类似变化。因此,动脉的膨胀压力基本上保持不变,就像静脉的膨胀压力一样。颅内压的初次升高会使脑静脉通道的流出量收缩。同时,压力的增加往往会引起动脉血管的扩张,正如刚才提到的。然而,如果动脉血压上升,这后一种效应可能会被抵消。适度诱导的颅内压升高对脑血管阻力的净影响可能很小。还没有关于颅内压初级升高对 CBF 和 CMRO2 影响的实验研究报告。然而,间接证据表明,当颅内压升高 5-10 分钟至约 500mmH2O 时,脑循环仍然充足(349)。本综述后面将讨论与脑瘤相关的颅内压增高患者的脑循环问题。
The vasomotor activity of the intracranial vessels constitutes the decisive intrinsic regulator of the cerebrovascular resistance. One important type of vasomotor activity has already been discussed, i.e., the variations in diameter of the cerebral arteries due to pressure changes. Equally important for the regulation of cerebrovascular resistance are chemical or humoral factors, whereas the role of neurogenic regulatory mechanisms remains, as we shall see, more dubious. The chemical and neurogenic control mechanisms will be discussed in the remainder of this section.
颅内血管的血管舒缩活性构成了脑血管阻力的决定性内在调节剂。已经讨论了一种重要类型的血管运动活动,即由于压力变化导致的脑动脉直径变化。对于脑血管阻力的调节同样重要的是化学或体液因素,而神经源性调节机制的作用仍然存在,正如我们将看到的,更加可疑。化学和神经源性控制机制将在本节的其余部分讨论。
# 二氧化碳
Carbon Dioxide
CO2 causes pronounced dilatation of the cerebral arterioles. This has been demonstrated repeatedly in animal studies employing a variety of techniques (350; see also 292, 318).
二氧化碳会导致大脑动脉血管的明显扩张。这在采用各种技术的动物研究中已被反复证明(350;也见 292,318)。
Quantitative data. In normal man, an increase of the alveolar and thus the arterial carbon dioxide tensions (PCO2) causes a striking increase in cerebral blood flow. Thus, hypercapnia induced by the inhalation of 5% CO2 increases cerebral perfusion by about 50 per cent, while 7% CO2 causes an increase of about 100 per cent (174, 197, 198, 249, 289). Using the indicator method, Gibbs, Maxwell and Gibbs found that 10% CO 2 also caused a comparable increase (no). No quantitative studies have been reported on the effect of higher CO2 concentrations. Conversely, subnormal alveolar and arterial pCO2 values cause a pronounced cerebral vasoconstriction. Hypocapnia produced by marked hyperventilation has been found to decrease cerebral blood flow to about 60 per cent of the resting value (171). It is interesting that this is the same low critical level of cerebral perfusion as was found in severe hypotension associated with clinical signs of cerebral hypoxia (81). This indicates that the cerebral symptoms produced by severe hyperventilation may be partially caused by cerebral hypoxia in addition to the more direct effect of the low arterial pCO2 on cerebral cells. A recent study by Patterson and associates suggests that the cerebral vasodilatation produced by hypercapnia is a threshold phenomenon occurring only when the inspired CO2 concentrations exceed 2.5% (249). This threshold corresponds to a rise in arterial pCO2 of about 4.5 mm Hg. In anesthetized dogs, however, Noel and Schneider found that changes of arterial pCO2 of 2 mm Hg caused variations of the arteriovenous oxygen difference indicative of changes of 8 to 10 per cent in cerebral blood flow (239). During inhalation of up to 7% CO2, as well as during marked hyperventilation, the cerebral arteriovenous oxygen difference varies inversely with the changes of cerebral blood flow, and the cerebral oxygen uptake remains essentially unchanged (46, 63, 66, 104, no, 116, 127, 171, 174, 197, 198, 241, 249)?
定量数据。在正常人中,肺泡和动脉二氧化碳张力(PCO2)的增加会导致脑血流量的显著增加。因此,通过吸入 5% 的二氧化碳引起的高碳酸血症使大脑灌注量增加了大约 50%,而 7% 的二氧化碳会引起大约 100% 的增加(174, 197, 198, 249, 289)。吉布斯、麦克斯韦和吉布斯使用指标法发现,10% 的 CO 2 也会引起相当的增加(没有)。没有关于更高的二氧化碳浓度的影响的定量研究报告。相反,低于正常的肺泡和动脉 pCO2 值会引起明显的脑血管收缩。由明显的过度通气产生的低碳酸血症已被发现会使脑血流量减少到静止值的 60% 左右(171)。有趣的是,这与在伴有脑缺氧临床症状的严重低血压中发现的脑灌注低临界水平相同(81)。这表明由严重低通气产生的脑部症状,除了低动脉 pCO2 对脑细胞更直接的影响外,还可能部分由脑缺氧引起。Patterson 和他的同事最近的一项研究表明,由高碳酸血症产生的脑血管扩张是一种阈值现象,只有当吸入的二氧化碳浓度超过 2.5% 时才会发生(249)。这个阈值相当于动脉 pCO2 的上升约 4.5mmHg。然而,在麻醉的狗身上,Noel 和 Schneider 发现,动脉 pCO2 的变化为 2 毫米汞柱,引起动静脉氧差的变化,表明脑血流的变化为 8% 到 10%(239)。在吸入高达 7% 的二氧化碳时,以及在明显的过度通气时,脑动脉血氧差与脑血流的变化成反比,而脑氧摄取量基本上保持不变(46, 63, 66, 104, no, 116, 127, 171, 174, 197, 198, 241, 249)?
Mechanism of action. It is generally believed that the concentration of carbon dioxide—the pCO2—is in itself the decisive factor, and that concomitant changes of pH or the bicarbonate concentration play a secondary role or no role at all. Schieve and Wilson have clearly demonstrated in clinical experiments that CO 2 acts independently of moderate changes of pH (288). No clearcut data are available to distinguish the action of pCO2 from that of associated changes of the bicarbonate concentration.
作用机制。一般认为,二氧化碳的浓度 --pCO2 本身就是决定性的因素,而同时发生的 pH 值或碳酸氢盐浓度的变化起次要作用或根本不起作用。 Schieve 和 Wilson 在临床实验中清楚地证明,CO 2 的作用与 pH 值的适度变化无关(288)。目前还没有明确的数据可以将 pCO2 的作用与相关的碳酸氢盐浓度变化区分开来。
4 Kety and Schmidt (171) found a tendency to an increase in CMRO2 during hyperventilation. A possible explanation of this finding is given in the section on cerebral blood flow and oxygen uptake in disease states.
4 Kety 和 Schmidt (171) 发现在过度通气时 CMRO2 有增加的趋势。在疾病状态下的脑血流和摄氧量一节中给出了对这一发现的可能解释。
Increased arterial CO2 concentration results in relaxation of the intrinsic myogenic tone of the smooth muscle cells of the walls of the cerebral vessels. The fact that subnormal pCO2 values cause cerebral vasoconstriction may be taken as evidence for a kind of tonic relaxing influence exerted by the normal pCO2 level. There is little doubt that CO2 causes cerebral vasodilatation by some local action. This conclusion was reached by Wolff on the basis of animal experiments demonstrating that the dilatation by CO 2 was unaffected by interrupting all the known nervous pathways which could possibly affect the cerebrovascular resistance, i.e., sectioning of the cervical sympathetic nerve, the cranial nerves VI, VII and VIII, the spinal cord or the brain stem (348). The mechanism of this local action is not known. The above mentioned animal studies do not rule out the possibility that CO2 acts via local perivascular nervous structures. The observation that CO 2 will relax isolated strips of the wall of the carotid artery favors the hypothesis that CO 2 acts directly on the smooth muscle cells of the vessel walls (53). It is probable that CO2 reaches the smooth muscle cells by diffusion either from the blood or directly from the surrounding tissues.
动脉二氧化碳浓度的增加导致脑血管壁的平滑肌细胞的内在肌张力的放松。亚正常的 pCO2 值导致脑血管收缩的事实可以被认为是正常 pCO2 水平施加的一种强直性放松影响的证据。毋庸置疑,二氧化碳通过某种局部作用引起脑血管舒张。这一结论是 Wolff 在动物实验的基础上得出的,实验表明,中断所有可能影响脑血管阻力的已知神经通路,即切断颈交感神经、颅神经 VI、VII 和 VIII、脊髓或脑干,都不会影响 CO 2 的扩张(348)。这种局部作用的机制尚不清楚。上述动物研究并不排除二氧化碳通过局部血管周围神经结构发挥作用的可能性。观察到 CO 2 会使颈动脉壁的孤立条带放松,这有利于假设 CO 2 直接作用于血管壁的平滑肌细胞(53)。二氧化碳很可能通过扩散从血液或直接从周围组织到达平滑肌细胞。
Physiological importance. The obvious net effect of CO 2 is that of cushioning the sensitive cerebral tissues against the harmful effects of marked variations of the arterial pCO2- Arterial hypercapnia, by increasing cerebral perfusion, facilitates the disposal of CO 2 produced by the brain, and thus the cerebral venous PCO2 is raised less above its normal level than the arterial pCO2. Conversely, in arterial hypocapnia the decrease of cerebral perfusion restricts the CO 2 loss from the brain, and for this reason the cerebral venous pCO2 is less decreased than the arterial. This damping of the excursions of the cerebral venous pCO2 probably reflects a similar damping of the pCO2 of the cerebral tissues. The beneficial effect of such a homeostatic control of the tissue pCO2 is illustrated by the fact that both high and low tissue pCO2 values have a noxious effect on the brain. High tissue pCO2 values cause depression of mental functions, as exemplified by the coma resulting from the inhalation of 30% CO 2 in normal man (219), and the confusion or coma due to CO 2 retention which may be caused by a reduction of pulmonary ventilation by oxygen inhalation in patients with severe pulmonary insufficiency (250). Low values of pCO2 in the cerebral tissues have presumably also a depressant effect on the cerebral functions, according to studies by Gibbs and co-workers, which showed that hypocapnia per se may cause derangement of the mental and electrical activities of the cerebral cortex (108).
* 生理上的重要性。*CO 2 的明显净效应是缓冲敏感的脑组织,使其免受动脉 pCO2 明显变化的有害影响。 动脉高碳酸血症通过增加脑灌注,促进了大脑产生的 CO 2 的处理,因此,脑静脉 PCO2 比动脉 pCO2 的正常水平提高得少。相反,在动脉低碳酸血症中,脑灌注的减少限制了大脑中 CO 2 的流失,因此,脑静脉 PCO2 的下降幅度小于动脉。这种对脑静脉 pCO2 波动的抑制可能反映了对脑组织 pCO2 的类似抑制。高和低的组织 pCO2 值都会对大脑产生有害的影响,这一事实说明了组织 pCO2 的这种平衡控制的有益作用。高的组织 pCO2 值会导致精神功能的抑制,例如正常人吸入 30% 的 CO 2 导致的昏迷(219),以及严重肺功能不全的病人吸入氧气导致肺部通气量减少而引起的 CO 2 潴留导致的混乱或昏迷(250)。根据 Gibbs 和同事的研究,脑组织中的 pCO2 低值可能对脑功能也有抑制作用,研究表明,低碳酸血症本身可能导致大脑皮层的精神和电活动失调(108)。
CO 2 is a more powerful cerebral vasodilator than any other substance yet studied. Also, CO2 is the main product of cerebral metabolism. These facts, combined with the local site of action of CO2, form the basis for a widely accepted theory concerning the physiological role of CO 2 in the homeostatic regulation of cerebral perfusion according to the metabolic needs of the tissues: An increase of function in a local nervous center causes an increase of oxidative metabolism, and hence an increased CO2 production; this causes a local rise of tissue pCO2 and local vasodilatation; the increased perfusion of the area tends to sustain the increased metabolism and to maintain the chemical milieu of the tissue. The opposite chain of events may follow a decrease of function and metabolism (50, go, 158, 292, 296, 34^)- Various proponents of this theory have stressed that the local adjustment of perfusion to metabolism may be due not only to CO2, but also to other vasodilator products of metabolism (see e.g. 292).
二氧化碳是一种比目前研究的任何其他物质更强大的脑血管扩张剂。而且,二氧化碳是大脑代谢的主要产物。这些事实,再加上二氧化碳的局部作用部位,构成了一个被广泛接受的理论基础,该理论涉及 CO 2 在根据组织的代谢需要对脑灌注进行平衡调节方面的生理作用。局部神经中枢功能的增加导致氧化代谢的增加,从而增加了二氧化碳的产生;这导致了局部组织 pCO2 的上升和局部血管的扩张;该区域的灌注量的增加倾向于维持增加的代谢和保持组织的化学环境。相反的事件链可能是在功能和代谢下降后发生的 (50, go, 158, 292, 296, 34^)-- 这一理论的各种支持者强调,局部灌注对代谢的调整可能不仅是由于二氧化碳,而且是由于代谢的其他血管扩张产物(见例如 292)。
Clinical implications. The cerebral circulatory response to CO 2 has been studied in a variety of clinical conditions. In diabetic coma (169) and arterial hypoxia (105, 174, 192) cerebral vasodilatation occurs in spite of hypocapnia. This indicates that in these extreme conditions the vasoconstriction of low pCO2 is overpowered by strong vasodilatory effects, probably acidosis and hypoxia in the two conditions respectively. In anesthesia and cerebrovascular disease the absolute increase in cerebral blood flow caused by CO 2 inhalation is somewhat less than that in normal man (289). However, relative to the reduced cerebral blood flow in both conditions the reaction to CO2 may be considered normal, since the induced increase of cerebral venous oxygen tension reaches the same level as in normal man. For this reason, and because of the great variability reported in literature, CO 2 responsiveness does not seem to be applicable as a test for disclosing fixed organic pathology of the walls of the cerebral vessels in the average case of cerebrovascular disease (63, 66, 190, 241, 289; see also the discussion of cerebral circulation in cerebral arteriosclerosis).
临床意义在各种临床情况下研究了脑循环对二氧化碳的反应。在糖尿病昏迷(169)和动脉缺氧(105,174,192)中,尽管有低碳酸血症,但仍会出现脑血管舒张。这表明在这些极端条件下,低 pCO2 的血管收缩被强烈的血管扩张作用所压制,可能是这两种情况下分别出现了酸中毒和缺氧。在麻醉和脑血管疾病中,吸入 CO 2 引起的脑血流的绝对增加要比正常人的少一些(289)。然而,相对于这两种情况下的脑血流减少,对二氧化碳的反应可以被认为是正常的,因为诱发的脑静脉氧张力的增加达到了与正常人相同的水平。由于这个原因,并由于文献中报道的巨大变异性,CO 2 反应性似乎不能作为披露脑血管疾病一般病例中脑血管壁的固定有机病变的测试(63,66,190,241,289;也见脑动脉硬化中的脑循环讨论)。
In clinical conditions where marked hyperventilation is causing cerebral sympoms, the inhalation of CO 2 in moderate concentrations would be expected to have an immediate beneficial effect. Stimulation of the cerebral circulation by CO 2 inhalation is also of value in hastening recovery from general anesthesia with volatile anesthetics. Moreover, it increases the tolerance to low oxygen tensions (108) and to positive radial acceleration (42, 43, 101, 218, 265, 340). The use of CO 2 inhalation in chronic cerebral vascular disease is impracticable, and presumably without use. In certain cases of acute cerebral vascular disease, however, CO2 may be of some benefit. CO2 has been widely used in resuscitation from asphyxia. But in this condition the cerebral vessels are already maximally dilated, and the brain pCO2 is elevated. The addition of CO2 to the inspired air in this situation is therefore not indicated, unless actual hypocapnia has been produced by prolonged hyperventilation. Conceivably, it might even have a noxious effect by raising the pCO2 in the brain to a depressant level.
在明显的过度通气导致脑交感的临床情况下,吸入适度浓度的 CO 2 预计会立即产生有益效果。通过吸入 CO 2 刺激脑循环,对加速从挥发性麻醉剂的全身麻醉中恢复也有价值。此外,它还能增加对低氧张力(108)和正径向加速度的耐受性(42,43,101,218,265,340)。在慢性脑血管疾病中使用 CO 2 吸入是不切实际的,估计也是没有用的。然而,在某些急性脑血管疾病的病例中,二氧化碳可能会有一些好处。二氧化碳已被广泛用于窒息复苏中。但是在这种情况下,脑血管已经最大限度地扩张,而且脑部的 pCO2 也升高了。因此,在这种情况下,在吸入的空气中加入二氧化碳是没有意义的,除非长时间的过度通气产生了实际的低碳酸血症。可以想象,它甚至可能通过提高大脑中的 pCO2 到抑制水平而产生有害的影响。
# 氧气
Oxygen
Inhalation of air mixtures of low oxygen tensions causes dilation of the pial arteries, whereas high oxygen tensions cause a moderate vasoconstriction (350). Thus, the effect of O2 is in the opposite direction to that of CO2. In man, inhalation of 8-10% O2 at atmospheric pressure causes a distinct increase in cerebral blood flow to about 40 per cent above the resting value. No change occurs in cerebral oxygen consumption, but the arterial pCO2 decreases as a result of a secondary hyperpnea (137, 174, 186). This hypocapnia was shown by Turner and associates to have no power to constrict the cerebral vessels in face of the anoxic stimulus (339)- These investigators found that the increase in cerebral blood flow due to hypoxia was not further increased by artificially maintaining the arterial pCO2 at about the control level. Moderate variations of oxygen tensions below and above the normal level do not affect the cerebral blood flow or metabolism (138, 246, 339)- This is presumably due to the fact that the dissociation curve for oxyhemoglobin is nearly horizontal at normal arterial oxygen tensions. Thus, such variations of oxygen tensions cause little change of the oxygen content of the arterial blood and of cerebral oxygen delivery. Oxygen tensions in inspired air mixtures of 0.8-1 .o atmosphere cause a small but significant decrease of cerebral perfusion without changing the cerebral oxygen uptake (63, 137, 174, 186). Patients with cerebrovascular disease show less variation of CBF following changes of the inspired oxygen tension than normal subjects (63, 138). However, this response may be considered adequate relative to the reduced cerebral blood flow in such patients, since the observations suggest that the induced changes of cerebral venous oxygen tension were of the same magnitude as in normal man (cf. the similar findings regarding the reactivity to CO2 in cerebrovascular disease).
吸入低氧张力的空气混合物会引起小动脉的扩张,而高氧张力会引起适度的血管收缩(350)。因此,O2 的影响与 CO2 的影响方向相反。在人类中,在大气压下吸入 8-10% 的氧气会使脑血流量明显增加,比静止时的数值高出约 40%。大脑耗氧量没有变化,但由于继发性的高呼吸,动脉 pCO2 会下降(137,174,186)。特纳和他的同事表明,面对缺氧刺激,这种低碳酸血症没有能力收缩脑血管(339)-- 这些研究者发现,通过人为地将动脉 pCO2 维持在大约控制水平上,不会进一步增加由于缺氧引起的脑血流的增加。低于和高于正常水平的适度的氧张力变化并不影响脑血流或代谢(138, 246, 339)-- 这可能是由于氧合血红蛋白的解离曲线在正常动脉氧张力下几乎是水平的。因此,氧张力的这种变化对动脉血的含氧量和脑部供氧量的变化很小。0.8-1.o 大气压的吸入空气混合物中的氧张力会导致脑灌注量小而明显的下降,而不会改变脑氧摄取量(63,137,174,186)。与正常人相比,脑血管疾病患者在吸入氧张力变化后表现出的 CBF 变化较小(63,138)。然而,相对于这些病人的脑血流减少,这种反应可以被认为是充分的,因为观察表明,诱发的脑静脉氧张力的变化与正常人的变化幅度相同(参考关于脑血管疾病中对二氧化碳反应性的类似发现)。
On the basis of all these observations and of similar results in animal studies, it appears that oxygen is of especial importance for the homeostatic regulation of cerebral perfusion in the emergency situation of severe anoxia of the brain (105, 292, 319). The pronounced vasodilatory response to oxygen lack means that a greater degree of arterial oxygen unsaturation can be tolerated than would be the case if this response did not occur. Consciousness is lost when the oxygen tension of the cerebral venous blood reaches 15-20 mm Hg, and at this level abnormal cortical electrical activity also starts abruptly (193, 194). It is interesting that the same critical level of cerebral venous oxygen tension has been found to limit the vasoconstriction of hypocapnia in animal experiments (239). Oxygen is generally thought to act on the cerebral vessels via local mechanisms just as does carbon dioxide (292). However, experimental evidence does not rule out the possible role of reflexes involving chemoreceptors (36).
根据所有这些观察和动物研究中的类似结果,在大脑严重缺氧的紧急情况下,氧气对大脑灌注的平衡调节似乎特别重要(105,292,319)。对缺氧的明显的血管舒张反应意味着可以容忍更大程度的动脉血氧不饱和度,而如果这种反应不发生的话。当脑静脉血的氧张力达到 15-20 毫米汞柱时,意识就会丧失,在这个水平上,异常的皮质电活动也突然开始(193,194)。有趣的是,在动物实验中发现同样的脑静脉血氧张力临界水平可以限制低碳酸血症的血管收缩(239)。一般认为氧气和二氧化碳一样,是通过局部机制作用于脑血管的(292)。然而,实验证据并不排除涉及化学感受器的反射的可能作用(36)。
Low arterial oxygen tensions cause mental symptoms before unconsciousness is reached, and such early symptoms are not associated with a measurable reduction of cerebral oxygen uptake (174). Possibly anoxia initially causes hypofunction only in small areas of the brain; but the contributory role of the secondary hypocapnia must also be considered (108).
动脉氧张力低在达到无意识之前就会引起精神症状,而这种早期症状与可测量的脑氧摄取量的减少无关(174)。可能缺氧最初只在大脑的小区域引起功能低下;但也必须考虑继发性低碳酸血症的贡献作用(108)。
Inhalation of 100 % O2 under a pressure of 3-4 atmospheres decreases cerebral blood flow moderately, does not change cerebral oxygen uptake, and causes only a slight increase in the pCO2 of cerebral venous blood (186). These observations indicate that the cerebral symptoms of oxygen toxicity are not caused by insufficient cerebral circulation or hypercapnia, but rather by a noxious effect of high oxygen tensions locally in the cerebral tissues. The inhalation of 100% O2 at a pressure of 1 atmosphere or less has been found useful in a variety of conditions. In a few instances, however, oxygen inhalation may have serious side effects. In premature infants it may lead to blindness, and in severe pulmonary failure it may cause a deleterious rise in pCO2 associated with a further rise in the already increased cerebral blood flow (250).
在 3-4 个大气压下吸入 100% 的氧气会适度减少脑血流量,不改变脑的摄氧量,只导致脑静脉血的 pCO2 轻微增加(186)。这些观察表明,氧中毒的脑部症状不是由脑循环不足或高碳酸血症引起的,而是由脑组织局部的高氧张力的有害影响引起的。在各种情况下,在 1 个大气压或更小的压力下吸入 100% 的氧气已被发现是有用的。然而,在少数情况下,氧气吸入可能有严重的副作用。在早产儿中,它可能导致失明,在严重的肺功能衰竭中,它可能导致有害的 pCO2 的上升,与已经增加的脑血流进一步上升有关(250)。
# 氢离子的浓度和葡萄糖
Hydrogen Ion Concentration and Glucose
The effect of variation of pH on the cerebral circulation in animals is not clear, although weak vasodilation by acidosis and mild vasoconstriction by alkalosis have been most commonly reported (292, 319). Schieve and Wilson studied moderate changes of pH in man and failed to demonstrate any effect beyond that which may be attributed to the concomitant changes of the carbon dioxide concentration (288). They found that mild acidosis caused by ammonium chloride infusion reduced arterial pCO2 and the cerebral blood flow, while mild alkalosis produced by bicarbonate infusion caused an increase of cerebral perfusion. In the latter studies the arterial pCCh was not reported, but it is likely that it was increased (317). Observations by Kety and associates, however, have been interpreted to indicate that acidosis may cause cerebral vasodilation in man (169). These authors studied patients in diabetic coma with marked acidosis and low arterial pCO2. The cerebral oxygen uptake was much reduced, while the cerebral blood flow was higher than normal. In these studies, the arterial pH was much lower than in the above mentioned studies of the effect of ammonium chloride. For this reason, it is entirely possible that the vasodilation in diabetic coma is caused by the severe acidosis. It cannot be ruled out, however, that other biochemical abnormalities may be of importance.
pH 值的变化对动物脑循环的影响尚不清楚,尽管最常见的报道是酸中毒造成的微弱血管扩张和碱中毒造成的轻度血管收缩(292,319)。Schieve 和 Wilson 研究了人体内 pH 值的适度变化,除了可能归因于同时发生的二氧化碳浓度变化外,未能证明有任何影响(288)。他们发现,由氯化铵输液引起的轻度酸中毒降低了动脉 pCO2 和脑血流,而由碳酸氢盐输液产生的轻度碱中毒引起了脑灌注的增加。在后者的研究中,没有报告动脉 pCCh,但很可能是增加了(317)。然而,Kety 和同事的观察结果被解释为表明,酸中毒可能导致人的脑血管扩张(169)。这些作者研究了有明显酸中毒和低动脉 pCO2 的糖尿病昏迷患者。大脑摄氧量大大降低,而脑血流量却高于正常水平。在这些研究中,动脉 pH 值比上述关于氯化铵影响的研究低得多。由于这个原因,糖尿病昏迷时的血管扩张完全有可能是由严重的酸中毒引起的。然而,也不能排除其他生化异常可能具有重要意义。
Glucose lack is presumably directly or indirectly a vasodilatory stimulus in hypoglycemic coma. In this condition, the arterial concentrations of carbon dioxide, oxygen and hydrogen ion are essentially unchanged, but the cerebral oxygen uptake is markedly reduced (176). As will be described in the following section, under such conditions the cerebral blood flow would be expected to be reduced pari passu with the decrease in oxygen uptake of the brain. Thus it is remarkable that the cerebral perfusion has been found to remain at the normal level (176), an observation suggesting the presence of a vasodilating influence.
在低血糖昏迷中,葡萄糖的缺乏可能直接或间接地成为血管扩张的刺激因素。在这种情况下,动脉中的二氧化碳、氧气和氢离子的浓度基本上没有变化,但脑的摄氧量却明显减少(176)。正如下一节所描述的那样,在这种条件下,脑血流量预计会随着大脑摄氧量的减少而减少。因此,值得注意的是,大脑灌注量被发现保持在正常水平(176),这一观察表明存在着血管扩张的影响。
# 脑代谢
Cerebral Metabolism
In 1914 Barcroft formulated the principle that increased activity of an organ results in enhanced oxidative metabolism and blood flow, while decreased activity reduces both factors (12). The brain of primates seems to conform to this principle, according to the studies on monkeys of Schmidt, Kety and Pennes (294). During induced convulsions the cerebral oxygen consumption and the cerebral blood flow increased in parallel fashion, while during anesthesia both values decreased proportionately. The tensions of carbon dioxide and oxygen in the cerebral venous blood remained fairly unchanged, indicating that the perfusion changes adequately compensated for the metabolic changes. As artificial ventilation was used in these monkey experiments, they cannot be taken to reflect directly the situation in spontaneous seizures in man, where marked arterial hypoxia develops. No adequate human studies made during convulsions have been reported. In an isolated observation of a spontaneous eclamptic seizure in a toxemic patient, McCall and Taylor found that the cerebral arteriovenous oxygen difference dropped to half the resting value (210). Unless the cerebral blood flow had actually quadrupled, the oxygen metabolism cannot have doubled during the seizure, as was the case in the monkey studies. Such a tremendous increase of cerebral perfusion is unlikely, and the observation, however isolated, suggests that the cerebral oxygen delivery may be insufficient to sustain a 100 per cent increase in cerebral oxygen metabolism during spontaneous seizure in man.
1914 年,Barcroft 提出了这样一个原则:一个器官活动的增加会导致氧化代谢和血流的增强,而活动的减少则会降低这两个因素(12)。根据 Schmidt、Kety 和 Pennes(294)对猴子的研究,灵长类动物的大脑似乎也符合这一原则。在诱导抽搐期间,脑耗氧量和脑血流量以平行的方式增加,而在麻醉期间,这两个值都按比例减少。大脑静脉血中的二氧化碳和氧气的张力保持相当的不变,表明灌注变化充分补偿了代谢变化。由于在这些猴子的实验中使用了人工通气,因此不能直接反映人类自发癫痫发作的情况,在这种情况下会出现明显的动脉缺氧。目前还没有关于在惊厥期间进行的充分的人类研究的报道。在对一个中毒病人的自发性癫痫发作的单独观察中,麦考尔和泰勒发现,脑动脉血氧差下降到静止值的一半(210)。除非脑血流量实际上增加了四倍,否则在发作期间,氧代谢不可能增加一倍,就像猴子研究中的情况那样。如此巨大的脑灌注量的增加是不可能的,而且这一观察,无论如何是孤立的,表明在人的自发发作期间,脑氧输送可能不足以维持 100% 的脑氧代谢的增加。
High values of cerebral metabolism and cerebral blood flow have been found in normal children (152) and during infusion of synthetic epinephrine (177). Numerous clinical studies have confirmed that decreased cerebral activity is accompanied by reduced cerebral oxygen uptake and, other factors being equal, a perfusion reduction which is proportionate to the reduction in oxygen uptake. This has been found in all studies of severe chronic brain disease and of acute cerebral disorders characterized by reduced consciousness. These studies will be discussed in detail later.
在正常儿童 (152) 和输注合成肾上腺素 (177) 期间,已经发现脑代谢和脑血流的高值。大量的临床研究证实,大脑活动的减少伴随着大脑摄氧量的减少,在其他因素相同的情况下,灌注量的减少与摄氧量的减少成正比。在所有对严重慢性脑病和以意识减退为特征的急性脑病的研究中都发现了这一点。这些研究将在后面详细讨论。
The regulation of cerebral perfusion according to the metabolic demand signifies that the chemical environment of the cerebral cells tends to remain unchanged. This important regulation of cerebrovascular resistance is presumably effected by a continuous interplay between chemical control mechanisms and the inherent tendency of the vessels to contract (292). Indirect evidence, already presented, strongly suggests that carbon dioxide and, in some conditions, oxygen are of prime importance in this control, although the possible role of other metabolites also must be kept in mind.
根据代谢需求对脑灌注的调节意味着脑细胞的化学环境倾向于保持不变。这种对脑血管阻力的重要调节可能是通过化学控制机制和血管固有的收缩趋势之间的持续相互作用来实现的(292)。已经提出的间接证据强烈地表明,二氧化碳和在某些条件下的氧气在这种控制中是最重要的,尽管其他代谢物的可能作用也必须铭记在心。
# 神经源性控制
Neurogenic Control
Anatomical studies have demonstrated perivascular nerve fibers accompanying the cerebral vessels both in man and in animals (214, 253, 334). The unmyelinated fibers are believed to mediate the neurogenic control of the cerebrovascular resistance, whereas the myelinated fibers are believed to be sensory afferents. These fibers are abundant in the adventitia of the major cerebral arteries, and Chorobski and Penfield have found nerve fibers even on intracerebral arterioles with a diameter of only 30-25 g (48).
解剖学研究表明,在人类和动物中,血管周围的神经纤维伴随着脑血管(214,253,334)。无髓纤维被认为是介导脑血管阻力的神经源控制,而有髓纤维被认为是感觉传入。这些纤维在主要脑动脉的内膜中很丰富,Chorobski 和 Penfield 甚至在直径只有 30-25 克的脑内动脉血管上发现了神经纤维(48)。
Sympathetic innervation. Arising mainly from the stellate and superior cervical ganglion, postganglionic sympathetic fibers form a continuous nervous plexus accompanying the internal carotid and vertebral arteries and their branches (48). In animal studies, Forbes and co-workers observed a feeble ipsilateral constriction of the pial arteries when the cervical sympathetic nerve was stimulated electrically, whereas stimulation of the stellate ganglion had no measurable effect (91, 94). Fog made similar observations, stressing that only the larger vessels showed any reactivity (82). Studies of local cerebral perfusion in animals during stimulation of the cervical sympathetic nerve have shown a decrease in perfusion in some areas of the brain, and no effect in other areas (201, 290, 291, 293, 295). Animal studies have also shown that when the cervical sympathetic nerve was cut, no vasodilatation or increase of perfusion occurred, not even in areas which responded to stimulation (82, 91, 94, 221, 293). Compared to the peripheral sympathetic innervation, that of the cerebral vessels may be characterized as being weak, inconsistent, and without tonic effect. As the cerebral vessels are highly reactive to other stimuli (chemical or pressure-induced), Schmidt has concluded that the sympathetic cerebral vasomotor innervation is probably without physiological importance (292). In man, no studies have been reported of the influence on cerebral blood flow of stimulations of the cervical sympathetic nerve. As will be discussed below, blocking or extirpation of the stellate ganglion does not change cerebral blood flow significantly in patients with or without acute cerebrovascular disease.
* 交感神经支配。* 主要来自星状神经节和颈上神经节,节后交感神经纤维形成一个连续的神经丛,伴随着颈内动脉和椎动脉及其分支(48)。在动物研究中,福布斯和同事们观察到,当颈部交感神经受到电刺激时,同侧的小动脉会出现微弱的收缩,而刺激星状神经节则没有可测量的效果(91,94)。Fog 做了类似的观察,强调只有较大的血管显示任何反应性(82)。在刺激颈交感神经时对动物局部脑灌注的研究表明,大脑某些区域的灌注量减少,而其他区域没有影响(201, 290, 291, 293, 295)。动物研究也表明,当颈交感神经被切断时,没有发生血管扩张或灌注增加,甚至在对刺激有反应的区域也没有(82,91,94,221,293)。与周围的交感神经支配相比,脑血管的交感神经支配可以说是微弱的、不一致的,而且没有强直作用。由于脑血管对其他刺激(化学或压力引起的)有高度反应,Schmidt 认为交感神经的脑血管运动支配可能没有生理意义(292)。在人类中,还没有关于刺激颈部交感神经对脑血流影响的研究报告。正如下文所讨论的,在有或没有急性脑血管病的病人中,阻断或切除星状神经节并不明显改变脑血流。
Parasympathetic innervation. Ghorobski and Penfield have traced unmyelinated nerve fibers from the facial nerve through the geniculate ganglion via the great superficial petrosal nerve to the pericarotid nerve plexus (48). Animal experiments have demonstrated a weak, ipsilateral cerebral vasodilation during faradic stimulation of the facial nerve (48, 92, 93). The physiological role of this parasympathetic vasodilator pathway is unknown, and no pertinent studies in man have been reported.
没有明显疾病迹象的非精神病老年受试者也被发现有类似的脑氧代谢率的降低(63,279,289),而经过高度筛选的、最正常的老年受试者没有显示出明显的降低(320)。 这些观察结果已经在关于年龄影响的章节中讨论过了,可以解释为许多非精神病患者的老年受试者在慢性脑部疾病的基础上有脑氧摄取量的降低。 这样看来,在以脑摄氧量降低为证据的弥漫性脑部疾病方面,老年精神病患者并不比许多同龄的警觉、理智的人受到更严重的影响。
Influence of vagus, aortic and sinus nerves. Observations of the diameter of the pial arteries have shown weak and inconsistent cerebral vasodilatation following stimulation of the vagus, aortic and sinus nerves (92). Studies by Fog, however, strongly suggest that a decrease of arterial blood pressure may have been implicated (82). Also, Schmidt and co-workers were unable to find changes of local cerebral perfusion during stimulation or following the cutting of these nerves (290, 291, 293, 295). No studies have been reported concerning the influence of these various nerves on the cerebral circulation in man.
在后一种情况下,脑功能低下的临床症状仅限于智力的不明显下降。 Fazekas 和他的同事对老年患者的脑循环和摄氧量的研究似乎支持这一假设(63,68)。 作者没有发现 "警觉的" 和 "困惑的" 老年患者之间的脑氧代谢有任何明显的差异。 两组患者的脑氧摄取量都有相同程度的减少。
Stellate block in apoplexy. Animal studies showed, as has been mentioned, that while stimulation of the cervical sympathetic nerve did produce moderate vasoconstriction in some cerebral areas, then stimulation of the stellate ganglion was without any effect, and cutting of the sympathetic nerve did not cause cerebral vasodilatation. In man, several groups of investigators have studied the cerebral circulatory effect of stellate block or stellectomy, particularly in patients with acute cerebrovascular accidents (9, 135, 199, 237, 272, 302, 307). In none of these studies, with a total of 91 subjects, was a significant change in cerebral blood flow found. Shenkin and co-workers found a reduction in cerebrovascular resistance when restudying 11 subjects a few days after bilateral stellectomy (302, 307). A similar reduction of resistance, however, was found by Lassen and Munck, who reexamined 10 subjects at an interval of days without any operative intervention or other attempt to change the clinical conditions (188). Thus it appears likely that changes of arterial pCO2, blood pressure, and the concentration of hemoglobin, can wholly account for the observations of Shenkin and co-workers. In two studies it was noted that subjects with low initial values for cerebral blood flow showed an increase following stellectomy or stellate block (199, 302). This cannot be taken to indicate a cerebral vasodilation caused by the therapeutic measure. In effect, the results may be explained solely by regression towards the mean, as described by Sir Francis Galton in 1886 (98).
* 卒中的星状体阻滞。* 如前所述,动物研究表明,虽然刺激颈部交感神经确实在某些脑区产生适度的血管收缩,但刺激星状神经节却没有任何作用,切断交感神经也不会引起脑血管扩张。在人类中,有几组研究者研究了星状神经阻断或星状神经切除的脑循环效应,特别是在急性脑血管意外患者中(9,135,199,237,272,302,307)。在这些研究中,总共有 91 名受试者,都没有发现脑血流的明显变化。Shenkin 和他的同事在双侧支架切除术后几天重新研究 11 名受试者时发现脑血管阻力减少(302,307)。然而,Lassen 和 Munck 发现类似的阻力减少,他们在没有任何手术干预或其他试图改变临床条件的情况下,间隔数日重新检查了 10 名受试者(188)。因此,动脉 pCO2、血压和血红蛋白浓度的变化似乎可以完全解释申金和同事们的观察结果。在两项研究中注意到,脑血流初始值较低的受试者在星形切除术或星形阻断术后出现了增加(199,302)。这不能被认为是由治疗措施引起的脑血管扩张。实际上,这些结果可能完全由向平均值回归来解释,正如弗朗西斯 - 高尔顿爵士在 1886 年所描述的那样(98)。
Meyer, Fang and Denny-Brown have recently reported an interesting study on the oxygen tension in the cerebral cortex of monkeys subjected to occlusion of the middle cerebral artery (221). It was found that cutting the cervical sympathetic nerve did not decrease the area of tissue anoxia, whereas such an effect was found following the inhalation of 100% O2 (or oxygen without carbon dioxide). This study would indicate that oxygen inhalation might be of value in apoplexy. However, studying the effect of inhalation of 50-100% O2 in 17 patients with apoplexy, Heyman and co-workers found no rise of the subnormal values for the oxygen uptake of the brain. The authors even felt that the inhalation of pure oxygen might be noxious in this condition, as the slight reduction of blood flow might favor propagation of local thrombotic processes.
Meyer、Fang 和 Denny-Brown 最近报告了一项关于大脑中动脉闭塞的猴子大脑皮层中氧气张力的有趣研究(221)。研究发现,切断颈部交感神经并没有减少组织缺氧的面积,而在吸入 100% 的氧气(或不含二氧化碳的氧气)后却发现有这样的效果。这项研究表明,吸入氧气可能对神经麻痹症有价值。然而,在研究对 17 名脑瘫患者吸入 50-100% 氧气的效果时,海曼和同事们发现大脑摄氧量的亚正常值没有上升。作者甚至认为,在这种情况下吸入纯氧可能是有害的,因为血流的轻微减少可能有利于局部血栓的传播。
The negative result of the many experimental attempts to find cerebral vasodilatation after stellate block in apoplexy is, of course, not decisive in evaluating the therapeutic results of the procedure. It does, however, stress the importance of objective clinical criteria. It would be of great value if future clinical studies of the therapeutic effect of stellate block would include untreated control series and also objective techniques of assessing the clinical improvement (196, i99. 335)-
当然,许多实验试图发现脑卒中星状体阻断后的脑血管扩张,其结果是负面的,这对评价该手术的治疗效果没有决定性意义。然而,它确实强调了客观临床标准的重要性。如果今后对星状动脉阻断治疗效果的临床研究能包括未经治疗的对照组和评估临床改善的客观技术,那将是非常有价值的(196, i99. 335)。
Concluding remarks. The role of neurogenic mechanisms in the physiological intrinsic control of cerebral circulation is still uncertain. The very fact that perivascular nerves are abundant in the brain favors the idea that they do also have a function. The many observations mentioned above have demonstrated that the cerebral vasomotor innervation via sympathetic or parasympathetic pathways is either absent or at least much less pronounced than the corresponding innervation of the peripheral circulation. Indeed, available data suggest that the cerebral circulation does not participate in the central control of peripheral resistance: induced hypotension and carbon dioxide inhalation cause a centrally induced constriction of the peripheral vessels (86-88, 259, 325); in both conditions cerebral vasodilatation occurs; peripheral vessels will when denervated remain unchanged or even dilate in these conditions.
* 结语。* 神经源机制在脑循环的生理性内在控制中的作用仍不确定。血管周围神经在大脑中很丰富,这一事实本身就有利于它们确实也有一定的功能。上面提到的许多观察表明,通过交感神经或副交感神经途径的脑血管运动神经支配要么不存在,要么至少比外周循环的相应神经支配要少很多。事实上,现有的数据表明,脑循环并不参与外周阻力的中枢控制:诱导性低血压和二氧化碳吸入会导致外周血管的中枢性收缩(86-88,259,325);在这两种情况下都会发生脑血管舒张;外周血管在这些情况下被剥夺神经后会保持不变甚至扩张。
The possibility of the involvement of the perivascular nerves in the local regulation of cerebral blood flow according to the perfusion pressure and variations in the metabolic activity of the tissues cannot be excluded. Such involvement, however, remains entirely speculative, as no relevant experimental data are available. Perhaps available techniques could be utilized in studying these problems. Thus it might be of interest to know if local cocainization of the brain surface would block or alter the vascular adaptation to variations of blood pressure, to a local increase in metabolism, or to local tissue anoxia.
不能排除血管周围神经根据灌注压力和组织代谢活动的变化参与局部脑血流调节的可能性。然而,由于没有相关的实验数据,这种参与仍然是完全推测的。也许可以利用现有的技术来研究这些问题。因此,我们可能有兴趣知道,大脑表面的局部可卡因化是否会阻止或改变血管对血压变化、局部代谢增加或局部组织缺氧的适应。
# 正常人大脑的摄氧量
Cerebral Oxygen Uptake in Normal Man
The normal brain consumes oxygen at an average rate of 3.5 cc per 100 gm per minute and has a total oxygen uptake of about 50 cc per minute (27, 61, 173, 188, 199, 262, 284). Thus, nearly 20 per cent of the oxygen taken up by the whole body at rest is utilized by the brain. Normal mental functions are uniquely dependent on an uninterrupted and ample oxygen supply. If cerebral oxygen delivery is arrested by stopping the cerebral circulation, consciousness is lost in a few seconds (264). It can be calculated that the amount of oxygen physically dissolved in the brain tissues would actually suffice to sustain the cerebral metabolism at its normal level for a similar short period of a few seconds (158). This agreement between physiological observations and theoretical calculations suggests that the aerobic metabolism of the brain must continue at its normal rate in order to preserve the mental functions. Quantitative studies in man lend substantial support to this suggestion. It has been repeatedly shown that when arterial hypoxia or arterial hypotension are carried to such an extreme that mental symptoms of cerebral hypoxia begin to develop, then the cerebral oxygen uptake is still not measurably decreased (81, 174, 229, 230). In other words, during the actual situation of measurement in the average subject this uptake seems to be very close to, if not identical with the minimal value compatible with normal cerebral function. The observation that the cerebral oxygen uptake continues unabated at the waking level during natural sleep indirectly supports this general statement (217). It is also noteworthy in the present context that no condition is known in which normal mental function is maintained in spite of a subnormal cerebral oxygen uptake.
正常大脑消耗氧气的平均速度为每 100 克 3.5 毫升 / 分钟,总摄氧量约为每分钟 50 毫升(27,61,173,188,199,262,284)。因此,整个身体在静止状态下所吸收的氧气有近 20% 被大脑所利用。正常的精神功能独特地依赖于不间断的和充足的氧气供应。如果通过停止脑循环来阻止脑部氧气的输送,意识会在几秒钟内丧失(264)。可以计算出,物理上溶解在脑组织中的氧气量实际上足以在几秒钟的类似短暂时间内维持脑部代谢的正常水平(158)。生理观察和理论计算之间的这种一致性表明,大脑的有氧代谢必须以其正常的速度继续进行,以保持精神功能。对人的定量研究为这一建议提供了大量支持。已经多次证明,当动脉缺氧或动脉低血压达到如此极端的程度,以至于开始出现脑缺氧的精神症状时,那么脑的摄氧量仍然没有明显的下降(81,174,229,230)。换句话说,在一般受试者的实际测量情况下,这种摄取量似乎非常接近,甚至与符合正常脑功能的最小值相同。观察到在自然睡眠期间,脑氧摄取量继续保持在清醒的水平上,这间接地支持了这个一般的说法(217)。在目前的情况下,还值得注意的是,没有一种情况是在脑氧摄取量不正常的情况下仍能保持正常的精神功能。
The fact that the brain normally seems to operate with a kind of minimal or basal level of total oxygen uptake requires some further comments. Available evidence supports the idea that under physiological conditions increased function of a local area of the brain may well occur, leading to a local increase in metabolism (103, 266, 293). However, total cerebral metabolism has been found to remain unchanged in most physiological conditions such as sleep (217), the resting waking state, and during intellectual effort (321). This could be an effect of heterogeneity of the brain with respect to function. Conceivably increased function in one cerebral area might cause a depression of function in other areas. It is also possible that the different physiological states of cerebral activity only represent functional and metabolic changes in rather limited cerebral areas, with no measurable effect on total oxygen consumption. Thus, the brain could be compared to an iceberg, most neuronal functions remaining below the surface of consciousness and maintaining a fairly constant rate and oxygen demand. Total cerebral oxygen uptake is increased above the resting level only in a few special conditions, such as during epinephrine infusion (177), during epileptiform seizures (294), and possibly also in some cases of extreme anxiety (161).
大脑在正常情况下似乎以一种最低或基本的总摄氧量水平运作,这一事实需要进一步的评论。现有的证据支持这样的观点:在生理条件下,大脑局部区域的功能增加很可能导致局部代谢的增加(103,266,293)。然而,在大多数生理条件下,如睡眠(217)、休息清醒状态和智力努力期间(321),总的大脑代谢被发现保持不变。这可能是大脑在功能方面的异质性的影响。可以想象,一个大脑区域的功能增加可能会导致其他区域的功能受到抑制。也有可能大脑活动的不同生理状态只代表相当有限的大脑区域的功能和代谢变化,对总耗氧量没有可测量的影响。因此,可以把大脑比作一座冰山,大多数神经元的功能保持在意识的表面以下,并保持相当稳定的速率和氧气需求。只有在少数特殊情况下,如输注肾上腺素时(177)、癫痫发作时(294),以及可能在某些极度焦虑的情况下(161),大脑总摄氧量才会高于静止水平。
A brief outline of the metabolism of the brain will be given in order to explain the fundamental role of oxygen. Oxidative glucose metabolism is the primary and indispensable source of energy for continuously resynthesizing energy-rich phosphate compounds in the brain (142, 319), and the cerebral respiratory quotient remains close to unity in all conditions so far studied (27, 107, 173, 186, 217, 322). The glucose uptake of the brain is about 5.5 mg per 100 gm per minute, or about 80 mg per minute for the total brain (107, 165, 284, 322, 351). This is slightly more than could be accounted for even if the total cerebral oxygen supply were utilized in aerobic glucose metabolism (142). The possibility cannot be excluded that analytical errors of the glucose determinations could be of sufficient magnitude to explain this discrepancy of glucose and oxygen uptake. Another possibility is that the nonoxidized glucose represents a kind of overflow of the initial anaerobic glycolytic process, producing an excess of lactate and pyruvate which escapes via the cerebral venous blood (142).
为了解释氧气的基本作用,我们将简要介绍一下大脑的代谢情况。葡萄糖的氧化代谢是大脑中不断重新合成富含能量的磷酸盐化合物的主要和不可缺少的能量来源(142,319),在迄今为止研究的所有条件下,大脑的呼吸商数都保持在接近统一的水平(27,107,173,186,217,322)。大脑对葡萄糖的摄取量约为每 100 克每分钟 5.5 毫克,或全脑每分钟约 80 毫克(107, 165, 284, 322, 351)。这比在有氧葡萄糖代谢中利用全部脑供氧量所占的比例略高(142)。不能排除葡萄糖测定的分析误差足以解释这种葡萄糖和氧摄取量的差异的可能性。另一种可能性是,非氧化葡萄糖代表了最初的无氧糖酵解过程的一种溢出,产生了过量的乳酸和丙酮酸,并通过脑静脉血排出(142)。
Although the cerebral capillaries are generally less permeable than other capillaries, this so called blood-brain barrier undoubtedly permits the transmural passage of a great variety of substances, of which many more than oxygen, carbondioxide and glucose are of fundamental importance for cerebral metabolic processes (102, 319). It appears reasonably certain, however, that the high and continuous energy demand of the brain is satisfied predominantly via aerobic glucose metabolism in man in physiological as well as in most pathological conditions.
尽管大脑毛细血管的渗透性通常比其他毛细血管要低,但这种所谓的血脑屏障无疑允许多种物质跨膜通过,其中除了氧气、二氧化碳和葡萄糖外,还有许多物质对大脑代谢过程具有根本的重要性(102,319)。然而,可以肯定的是,在生理和大多数病理情况下,大脑对能量的持续高需求主要是通过有氧葡萄糖代谢来满足的。
# 青年人的正常值
Normal Values in Young Adults
In normal young adults, examined by means of the inert gas method in the resting recumbent position, the cerebral oxygen uptake per 100 gm of brain (CMRO2) is, as already mentioned, on the average about 3.5 cc per minute (173, 188). Studies using the modification of Scheinberg and Stead have shown somewhat higher normal values of CMRCh, averaging about 3.6 to 3.8 (27, 61, 199, 262, 284). The possible reasons for this discrepancy have been discussed in the section on the inert gas method.
如前所述,在正常的年轻成人中,通过惰性气体法检查,每 100 克大脑的脑氧摄取量(CMRO2)平均约为每分钟 3.5 毫升(173,188)。使用 Scheinberg 和 Stead 修改的研究显示 CMRCh 的正常值略高,平均约 3.6 至 3.8(27,61,199,262,284)。这种差异的可能原因已在关于惰性气体方法的章节中讨论过。
Males and females have the same CMRO2 values (173, 188, 206, 320), and racial differences apparently do not exist (4, 27, 61, 173, 188, 199, 262, 284). In unilateral inert gas studies a considerable variation of the individual CMRO2 values have been found. Such studies have in most cases demonstrated a standard deviation of normal CMRO2 of 0.4 to 0.6 cc per 100 gm per minute. In bilateral studies, using the Kr85 modification, the spread of the normal CMRO2 in a small series of nine cases was less pronounced, the standard deviation of this function being only 0.2 cc per 100 gm per minute (234), a value significantly lower than could be accounted for on the basis of the increased number of analyses alone.
男性和女性的 CMRO2 值相同(173、188、206、320),种族差异显然不存在(4、27、61、173、188、199、262、284)。在单边惰性气体研究中,已经发现个人 CMRO2 值有相当大的变化。这类研究在大多数情况下显示正常 CMRO2 的标准偏差为 0.4 至 0.6cc/100gm/min。在双侧研究中,使用 Kr85 修改,在 9 个病例的小系列中,正常 CMRO2 的分布没有那么明显,这个功能的标准偏差只有 0.2 毫升 / 100 克 / 分钟(234),这个值明显低于仅根据增加的分析数量所能解释的。
When restudying unilateral CMRO2 in the same subject under the same external conditions, considerable day-to-day variations often occur (128, 146, 171, 180, 188, 234, 338). A series of such repeated unilateral studies in eight normal subjects, using the Kr85 technique, has been reported (188, 234). In these studies the standard deviation of the normal day-to-day variations of CMRO2 in the individual normal subject can be calculated to be about 0.5 cc per 100 gm per minute. It is of interest that this intra-individual day-to-day variation is of the same magnitude as the above mentioned interindividual variation in a group of normals. Repeated bilateral CMRO2 studies have so far only been reported in four normal subjects, showing only minor day-to-day variations of CMRO2 (234).
在相同的外部条件下重新研究同一受试者的单侧 CMRO2 时,经常会出现相当大的日间变化(128, 146, 171, 180, 188, 234, 338)。已经报道了在 8 个正常受试者中使用 Kr85 技术进行的一系列这样的重复单侧研究(188,234)。在这些研究中,可以计算出单个正常人的 CMRO2 的正常日变化的标准偏差为每分钟每 100 克约 0.5 毫升。值得注意的是,这种个体内的日常变化与上述一组正常人的个体间变化的程度相同。 到目前为止,只有四个正常人的重复双侧 CMRO2 研究报告,显示 CMRO2 的日常变化很小(234)。
The results obtained in a great number of clinical studies based on unilateral CMRO2 determinations using the inert gas method will be discussed in the following sections.
以下部分将讨论在大量临床研究中获得的结果,这些研究基于使用惰性气体方法的单侧 CMRO2 测定
# 年龄的影响
Influence of Age
In a recent study using the original nitrous oxide technique, the cerebral circulation and oxygen uptake of a large group of carefully selected normal aged male subjects, of an average age of 71, was studied (320). The mean value of the CMRO2 in this group was found to be 3.4 cc per 100 gm per minute, which was not significantly different from the average value of 3.5 cc per 100 gm per minute, obtained in a group of young normal adults studied simultaneously. A moderate decrease of CMRO2 with age has been found in other studies (279, 289), while an isolated study reports a marked decrease with age (63). It seems most likely that these divergent results were obtained by including among the aged subjects some cases with chronic degenerative brain diseases and subnormal CMRO2 values (66, g6, 190). This may also explain the finding of subnormal CMRO2 in healthy subjects close to 100 years of age (71). Unpublished studies by Lassen, Lane and Feinberg using the bilateral Kr85 technique have shown a small (9%), but significant reduction of cerebral oxygen uptake in a group of normal aged subjects of an average age of 72 years.
在最近的一项研究中,使用了原始的氧化亚氮技术,研究了一大群精心挑选的平均年龄为 71 岁的正常男性受试者的脑循环和摄氧量(320)。这组受试者的 CMRO2 平均值为每 100 克 3.4 毫升,与同时研究的一组年轻正常成年人的平均值每 100 克 3.5 毫升没有明显区别。其他研究发现 CMRO2 随着年龄的增长而适度下降(279,289),而一项单独的研究报告说随着年龄的增长而明显下降(63)。这些不同的结果似乎很可能是由于在老年受试者中包括了一些患有慢性退行性脑病和 CMRO2 值不正常的病例(66,g6,190)。这也可以解释在接近 100 岁的健康受试者中发现 CMRO2 不正常的情况(71)。Lassen、Lane 和 Feinberg 使用双侧 Kr85 技术进行的未发表的研究显示,在一组平均年龄为 72 岁的正常老年受试者中,脑氧摄取量有小幅(9%),但明显减少。
Considered as a whole, the available data suggest in the opinion of the reviewer a minor reduction of cerebral oxygen uptake per 100 gm brain in normal persons of about 70 years of age. A reduction of brain weight means a correspondingly lower value for total cerebral oxygen uptake. (Obviously this statement is valid in general regarding the results obtained by using the inert gas method; especially when evaluating the results in chronic brain disorders it is well to keep this point in mind.) The slight reduction of oxygen uptake per 100 gm brain in normal old age is presumably due to incipient chronic brain disease. The cause of this cerebral affliction of old age is obscure. Generalized cerebral vascular insufficiency is presumably not operative, since all the above mentioned studies have shown that the values for cerebral perfusion are proportionately no more reduced than those for oxygen uptake.
从整体上考虑,审查员认为现有的数据表明,在大约 70 岁的正常人中,每 100 克脑的摄氧量有轻微的减少。大脑重量的减少意味着总脑氧摄取量的相应降低。(显然,对于使用惰性气体方法所获得的结果,这一声明在一般情况下是有效的;特别是在评估慢性脑病的结果时,最好记住这一点)。在正常的老年人中,每 100 克大脑的摄氧量略有减少,这可能是由于初期的慢性大脑疾病造成的。老年的这种脑部疾病的原因是不明确的。普遍性的脑血管功能不全可能没有起作用,因为上述所有的研究都表明,脑灌注的数值在比例上并不比摄氧量的数值减少。
In childhood and adolescence the normal values for cerebral oxygen uptake are not firmly established. In vitro studies of the oxygen uptake of cerebral tissues of lower mammals have repeatedly shown low values at birth, a subsequent phase of high cerebral metabolic activity in young animals, followed by a decrease to the level of the adult animal (cf. 142). In man, two studies under nearly normal physiological conditions have been reported, using modifications of the inert gas method permitting reduction of the volume of blood sampled during the experiment (100, 152). In a study of children 2-3 years of age with various neurological diseases, a CMRO2 of the same level as in normal young adults were found in those children who had a normal mental development and only minor neurological disorders (100). In a more closely normal group of children about 5-10 years of age, Kennedy and associates have recently reported CMRO2 values about 5.0 cc per 100 gm per minute, which was considerably above the average value found in a group of normal young adults studied simultaneously (152). In these studies nitrous oxide was administered by means of a plastic dome and, as a result, the arterial curves continued to rise more than usually after 10 minutes of inhalation. It can be calculated that this may have introduced an error tending to give an overestimation of the CBF and CMRO2 of 5-10 percent (cf. page 187). This may explain why the young normal adult subjects studied by Kennedy and associates had somewhat high CMRO2 values. It cannot, however, explain the difference between the young adults and the children. This difference cannot be due to anxiety, since only cooperative and relaxed children were examined. If the data of Kennedy et al. are truely representative of the average level of CMRO2 in children, then the oxygen uptake of the brain in the middle of the first decade of life accounts for about 50 per cent of the total basal oxygen consumption of the body. These same investigators found that the CMRO2 of adolescents was also somewhat higher than that found in young adults (152).
在儿童和青少年时期,脑氧摄取量的正常值并不确定。对低等哺乳动物脑组织摄氧量的体外研究一再表明,出生时的数值较低,随后年轻动物的脑代谢活动较高,随后下降到成年动物的水平(参见 142)。在人类中,有两项研究在几乎正常的生理条件下被报道,使用惰性气体方法的修改,允许在实验中减少血液采样的体积(100,152)。在一项对患有各种神经系统疾病的 2-3 岁儿童的研究中,发现那些智力发育正常且只有轻微神经系统疾病的儿童的 CMRO2 与正常年轻人的水平相同(100)。在一组更接近正常的 5-10 岁的儿童中,肯尼迪和同事最近报告了 CMRO2 值约为每 100 克 5.0 毫升 / 分钟,这大大高于同时研究的一组正常年轻成人的平均值(152)。在这些研究中,一氧化二氮是通过塑料圆顶的方式给药的,因此,在吸入 10 分钟后,动脉曲线继续上升,超过了通常的水平。可以计算出,这可能引入了一个误差,倾向于高估 CBF 和 CMRO2 的 5-10%(参见第 187 页)。这可以解释为什么肯尼迪和同事研究的年轻正常成人受试者的 CMRO2 值有点高。然而,它不能解释年轻成人和儿童之间的差异。这种差异不可能是由于焦虑造成的,因为只检查了合作和放松的儿童。如果肯尼迪等人 * 的数据真的能代表儿童 CMRO2 的平均水平,那么在生命的第一个十年中,大脑的摄氧量约占身体基础耗氧总量的 50%。这些调查人员还发现,青少年的 CMRO2 也比青壮年高一些(152)。
It may be mentioned that in childhood as well as in senescence the cerebral blood flow varies in parallel with the cerebral oxygen uptake. Thus, the arteriovenous oxygen difference of the brain remains relatively constant, as do the cerebral venous oxygen and carbon dioxide tensions also. Insofar as these tensions can be taken to represent those of the brain, these observations suggest that the chemical milieu of the cerebral tissues is maintained fairly constant throughout life.
值得一提的是,在儿童期和衰老期,脑血流量的变化与脑氧摄取量的变化同步。因此,大脑的动静脉氧差保持相对恒定,脑静脉的氧气和二氧化碳的张力也是如此。只要这些张力可以被视为代表大脑的张力,这些观察表明,大脑组织的化学环境在整个生命过程中保持相当稳定。
# 大脑功能生理变化的影响
Influence of Physiological Variations of Cerebral Function
The lack of change of cerebral oxygen uptake in physiological conditions characterized by variations of cerebral function has already been discussed. These important findings deserve a more detailed presentation, to be given below.
在以脑功能变化为特征的生理条件下,脑氧摄取量没有变化,这一点已经讨论过了。这些重要的发现值得更详细的介绍,将在下面给出。
Intellectual effort. Normal values of cerebral perfusion and oxygen metabolism have been obtained in the resting waking state without regard to the mental activity of the subject. The influence of concentrated intellectual effort has been studied in young normal adults (321). Shortly after a control study, the test subjects were required to solve mentally a series of fairly simple arithmetic problems. No significant change of CMRO2 or cerebral perfusion and vascular resistance was found.
* 脑力劳动。* 脑灌注和氧代谢的正常值是在静止的清醒状态下获得的,不考虑受试者的精神活动。在年轻的正常成年人中,已经研究了集中智力的影响(321)。在进行对照研究后不久,要求测试对象用脑解决一系列相当简单的算术问题。没有发现 CMRO2 或脑灌注和血管阻力的明显变化。
Physical exercise. Moderate muscular activity has been found to have no influence on the CMRO2, whereas the cerebral blood flow was slightly decreased, presumably as a result of mild hypocapnia (182).
* 体育锻炼。* 适度的肌肉活动已被发现对 CMRO2 没有影响,而脑血流略有下降,可能是由于轻度的低碳酸血症(182)。
Apprehension. Apprehension is in this context taken to mean an acute condition of subjective and objective signs of anxiety, fear and discomfort during the actual test situation of a person of no apparent emotional instability prior to the test. In a series of such observations in normal subjects, no significant effect of apprehension was found (284). An isolated observation by Kety has suggested that severe apprehension may cause a marked rise in cerebral oxygen uptake (161). It was suggested that this rise in oxygen uptake might be due to the stimulating action of Z-epinephrine on cerebral metabolism (177).
忧虑。 忧虑在这里被认为是指在测试前没有明显情绪不稳定的人在实际测试情况下出现的焦虑、恐惧和不舒服的主观和客观迹象的急性状况。在对正常受试者进行的一系列此类观察中,没有发现忧虑的明显影响(284)。Kety 的一项孤立的观察表明,严重的忧虑可能导致大脑摄氧量的明显上升(161)。有人认为,这种摄氧量的上升可能是由于 Z - 肾上腺素对脑部代谢的刺激作用(177)。
Sleep. In a painstaking study, the influence of normal sleep has been studied (217). Only those normal subjects who managed to fall asleep spontaneously with needles in place and an anesthesia mask on, and who had electroencephalographic evidence of sleep, were accepted in the study. No change in cerebral oxygen uptake was found compared to the presleep control studies in the fatigued waking state on the same subjects. Fatigue alone was shown to be without effect in another series of subjects. The cerebral blood flow increased slightly during sleep, presumably due to a mild hypercapnia. These observations are of interest in relation to various theories of the nature of natural sleep. The possibility that generalized cerebral ischemia was involved can be excluded. These studies also appear to rule out the hypothesis that sleep is a kind of endogenous narcosis with a decreased over-all metabolism permitting the replenishment of certain substrate stores presumably depleted by the active metabolism of the waking state. As will be discussed in the next section, narcosis and other forms of coma are all characterized by a marked reduction of cerebral oxygen uptake. The observation that cerebral metabolism goes on unabated during sleep may be taken to indicate that the difference between sleep and the waking state is not so fundamental as one might believe.
* 睡眠。* 在一项艰苦的研究中,对正常睡眠的影响进行了研究(217)。只有那些在打针和戴着麻醉面罩的情况下能够自动入睡,并且有脑电图证据的正常受试者才被纳入研究范围。与睡眠前的对照研究相比,在同一受试者的疲劳觉醒状态下,没有发现脑氧摄取量的变化。在另一个系列的受试者中,单独的疲劳被证明是没有影响的。睡眠期间脑血流量略有增加,可能是由于轻度的高碳酸血症。这些观察与自然睡眠性质的各种理论有关。可以排除全身性脑缺血的可能性。这些研究似乎也排除了这样的假设,即睡眠是一种内源性麻醉,整体代谢下降,允许补充某些底物储存,而这些底物可能被清醒状态下的积极代谢耗尽。正如下一节将讨论的那样,麻醉症和其他形式的昏迷都以脑氧摄取量的明显减少为特征。观察到大脑的新陈代谢在睡眠期间有增无减,这可以表明睡眠和清醒状态之间的差异并不像人们所认为的那么根本。
But apart from this, the study does not give any clues to the enigma of why we must sleep.
但除此之外,这项研究并没有为我们为什么必须睡觉的谜团提供任何线索。
Other conditions. As mentioned in the section on the regulation of cerebral blood flow, physiological variations of the respiratory gas tensions of the arterial blood and of the perfusion pressure of the brain do not change the oxygen uptake of the brain.
* 其他条件。* 正如在脑血流调节一节中提到的,动脉血的呼吸气体张力和大脑灌注压力的生理变化并不改变大脑的摄氧量。
The effect of low body temperatures has been studied mostly in animal experiments. The cerebral oxygen uptake and the cerebral perfusion are reduced roughly in proportion to the reduction in total body oxygen uptake, cardiac output, pulse rate, and myocardial and renal blood flow. These values all decrease to about 50 per cent of the normal levels at a temperature of 28°C (134, 222, 263, 296). At about this temperature the cerebral function is depressed to a level corresponding to that of surgical anesthesia (cold anesthesia). Similar results were obtained in a study of CBF and CMRO2 in man, using a combination of physical cooling and a variety of pharmacological agents (artificial hibernation) (77).
低体温的影响主要在动物实验中进行研究。大脑摄氧量和大脑灌注量的减少大致与全身摄氧量、心输出量、脉搏、心肌和肾脏血流的减少成正比。这些数值在温度为 28℃时都下降到正常水平的 50% 左右(134, 222, 263, 296)。在大约这个温度下,大脑功能被抑制到相当于手术麻醉(冷麻醉)的水平。在对人的 CBF 和 CMRO2 的研究中,使用物理冷却和各种药物制剂(人工冬眠)的组合,也得到了类似的结果(77)。
High body temperatures of about 39 °C induced by pyrogen injection have been studied in patients with asymptomatic neurosyphilis and with dementia paralytica (140). An increase of cerebral oxygen uptake of 3-24 per cent was found in the two groups respectively. Only the change of 24 per cent was found to be statistically significant. It may be mentioned, however, that the changes observed in both groups seem to be compatible with the hypothesis that the hyperpyrexia had actually caused a 10-15 per cent increase of CMRO2 in both groups. A change of this magnitude would be expected to occur, on the basis of the results reported in hypothermia. No studies have been made of cerebral metabolism in fever with mental symptoms. That the cerebral function is severely or even irreversibly affected by extreme hyperpyrexia is well established clinically. The nature of this effect is unknown.
在无症状的神经梅毒患者和瘫痪性痴呆患者中研究了通过注射热原诱导的约 39℃的高体温(140)。发现两组患者的脑氧摄取量分别增加了 3-24%。只有 24% 的变化被发现具有统计学上的意义。然而,可以提及的是,在两组中观察到的变化似乎与高热症实际上导致两组中的 CMRO2 增加 10-15% 的假设相一致。根据低体温报告的结果,这种程度的变化是可以预期的。没有对发热伴有精神症状的脑代谢进行过研究。脑功能受到极端高热的严重影响,甚至是不可逆转的影响,这在临床上已经得到证实。这种影响的性质尚不清楚。
# 疾病状态下的脑血流和摄氧量
Cerebral Blood Flow and Oxygen Uptake in Disease States
The finding of a subnormal cerebral oxygen uptake in a number of disease states may well be considered the most important knowledge gained from the many clinical studies of the circulation and metabolism of the brain. The grey matter of the hemispheres, of which the cerebral cortex forms by far the bulk, has a considerably higher oxygen consumption than the white matter. For this reason, it may be assumed that a subnormal cerebral oxygen uptake signifies a hypometabolism of the cerebral cortex. It is thus not surprising that a subnormal cerebral oxygen uptake is found only in conditions with distinct signs of diffuse hypofunction of the cerebral cortex. Two different types of such a hypofunction may be discerned: z) acute cerebral depression with a reduction of the level of consciousness, i.e., semicoma and coma; and 2) chronic cerebral degenerative diseases with a reduction of intellectual faculties, i.e., organic dementia. The following section will first review the literature concerning cerebral perfusion and oxygen metabolism in these two types of brain disease. Particular mention will be made of the relation of chronic brain disease to cerebral arteriosclerosis and to psychosis in elderly patients. Finally, various other neuropsychiatric disorders and a variety of systemic diseases will be discussed.
在一些疾病状态下发现脑氧摄取量不正常,这很可能被认为是对大脑循环和代谢的许多临床研究中获得的最重要的知识。半球的灰质(其中大脑皮层占大部分)比白质的耗氧量高得多。由于这个原因,我们可以认为,大脑摄氧量不正常意味着大脑皮层的新陈代谢不足。因此,只有在大脑皮层弥漫性功能低下的情况下,才会发现脑氧摄取量低于正常值,这并不令人惊讶。这种功能低下有两种不同的类型:Z)急性脑萎缩,意识水平下降,即半昏迷和昏迷;以及 * 2)* 慢性脑退化性疾病,智力下降,即器质性痴呆。下一节将首先回顾有关这两种类型的脑部疾病的脑灌注和氧代谢的文献。将特别提到慢性脑病与脑动脉硬化的关系,以及与老年患者精神病的关系。最后,将讨论其他各种神经精神疾病和各种系统性疾病。
# 不同病因不同程度的昏迷
Semicoma and Coma of Varying Etiology
In all conditions of semicoma or coma which have been studied—whether due to anesthetics, acute hypoglycemia, apoplexy, or any other cause—the reduction of consciousness correlates roughly with the decrease of cerebral oxygen uptake, regardless of the cause of the acute cerebral disorder (table 1). This correlation was first noted by Kety, who stated: “In all of our studies we have been impressed with the close correlation between the level of consciousness and the rate of oxygen consumption by the brain. In patients who are comatose for whatever reason, cerebral oxygen consumption falls to a value of less than 2.0 cc per 100 gm per minute, while in those who are semistuperous or confused, the value lies between 2.5 and 3.0” (156).
在所有已经研究过的半身不遂或昏迷的情况下 -- 不管是由于麻醉剂、急性低血糖、神经麻痹或任何其他原因 -- 意识的降低与脑氧摄取的减少大致相关,不管急性脑部疾病的原因是什么(表 1)。这种相关性是由 Kety 首先指出的,他说。"在我们所有的研究中,我们对意识水平和大脑耗氧率之间的密切关联印象深刻。在因任何原因而昏迷的病人中,脑耗氧量下降到每分钟每 100 克少于 2.0 毫升,而在那些半昏迷或意识模糊的病人中,这个数值在 2.5 和 3.0 之间"(156)。
Apart from this interesting observation, however, the many studies listed in table 1 have not shed any new light on the pathophysiology of coma. Generally the cerebral blood flow seems to be adequate in coma, as the relative reduction in perfusion is no greater than that of oxygen metabolism (in cerebral circulatory failure a disproportionate drop of perfusion is found; refs. 81, 154). In less marked forms of acute cerebral hypofunction than semicoma and coma, the cerebral oxygen uptake is not decreased significantly. The cerebral oxygen uptake is not measurably reduced in subjects with clinical signs of impending cerebral hypoxia caused by arterial hypotension (81), and in subjects with symptoms of cerebral depression due to hyperventilation (174) or the inhalation of 100% O2 under a pressure of several atmospheres (186). Similarly, barbiturate sedation does not depress cerebral oxygen uptake significantly (176, 210). It is possible, however, that the use of more accurate techniques and appropriate correction for the increased effect of heterogeneous perfusion upon the inert gas method would make it possible to demonstrate a reduction of cerebral oxygen consumption in one or more of these conditions.
然而,除了这一有趣的观察之外,表 1 所列的许多研究并没有对昏迷的病理生理学提供任何新的启示。一般来说,昏迷时脑血流似乎是充足的,因为灌注量的相对减少不超过氧代谢的减少(在脑循环衰竭时,发现灌注量的下降不成比例;参考文献。81, 154). 在比半身不遂和昏迷更不明显的急性脑功能低下的形式中,脑氧摄取量没有明显下降。在有动脉低血压引起的即将发生脑缺氧的临床症状的受试者(81),以及因过度通气(174)或在几个大气压下吸入 100% 氧气(186)而出现脑抑制症状的受试者中,脑氧摄取量没有明显减少。同样,巴比妥类镇静剂也不会明显抑制脑氧摄取量(176,210)。然而,使用更精确的技术和对惰性气体法中异质灌注的影响的适当修正,有可能证明在这些条件中的一种或多种情况下脑氧消耗的减少。
Table 1. Cerebral oxygen uptake in various types of coma
表一:不同类型昏迷中的脑氧摄取量
| TYPE OF COMA | CEREBRAL O2 UPTAKE cc/100 gm/min. | REF. |
|---|---|---|
| Normal subjects | 3.4 | 65, 173 |
| Intoxication* | ||
| Barbiturate intoxication (coma) | 2.3 | 65 |
| Barbiturate anesthesia | 2.1 | 19, 145, 289, 343 |
| Ethyl alcohol coma | 1.6 | 13 |
| Methyl alcohol coma | 2.0 | 14 |
| Steroid anesthesia | 1.7 | 115 |
| Artificial hibernation | 2.2 | 22, 77, 119, 316 |
| Uremic coma | 2.2 | 139 |
| Hepatic coma | 1.7 | 72, 342 |
| Damage and edema* | ||
| Irreversible post-hypoglycemic coma | 1.5 | 64 |
| Irreversible post-anoxic coma | 1.8 | 65 |
| Post-traumatic coma | 1.8 | 65 |
| Coma after craniotomy | 1.9 | 301 |
| Tumor cerebri with coma | 2.5 | 175 |
| Apoplexy with coma | 2.1 | 65 |
| Lack of nutrients* | ||
| Hypoglycemic coma | 1.9 | 176 |
| Secondary shock with coma | 1.9 | 69 |
* Presumed pathophysiological mechanism.
| 昏迷类型 | 大脑 O2 摄取 cc/100 gm/min. | REF. |
|---|---|---|
| 正常人 | 3.4 | 65, 173 |
| 中毒 * | ||
| 巴比妥酸盐中毒(昏迷) | 2.3 | 65 |
| 巴比妥酸盐麻醉 | 2.1 | 19, 145, 289, 343 |
| 乙醇昏迷 | 1.6 | 13 |
| 甲醇昏迷 | 2.0 | 14 |
| 类固醇麻醉 | 1.7 | 115 |
| 人工休眠 | 2.2 | 22, 77, 119, 316 |
| 尿毒症昏迷 | 2.2 | 139 |
| 肝昏迷 | 1.7 | 72, 342 |
| 损伤和水肿 * | ||
| 不可逆转的低血糖后昏迷 | 1.5 | 64 |
| 不可逆转的缺氧后昏迷 | 1.8 | 65 |
| 创伤后昏迷 | 1.8 | 65 |
| 开颅手术后昏迷 | 1.9 | 301 |
| 脑肿瘤昏迷 | 2.5 | 175 |
| 脑瘫昏迷 | 2.1 | 65 |
| 营养物质缺乏 * | ||
| 低血糖昏迷 | 1.9 | 176 |
| 休克继发昏迷 | 1.9 | 69 |
* 推定的病理生理学机制。
As mentioned in the chapter on the inert gas method, the heterogeneity of the cerebral perfusion may be expected to cause a greater error in low values of cerebral perfusion than in normal values. For this reason, the values for cerebral blood flow and oxygen uptake in severe hypotension and hyperventilation are relatively too high. This could be the explanation of the finding of an increase of cerebral oxygen uptake in 9 out of 12 hyperventilating subjects (174), and of the lack of reduction in severe hypotension with quite pronounced symptoms of cerebral hypoxia (81).
正如在惰性气体法一章中提到的,脑灌注的异质性可能会导致脑灌注的低值比正常值的误差更大。由于这个原因,在严重低血压和过度通气的情况下,脑血流和摄氧量的数值相对过高。这可能是对 12 个通气不足的受试者中 9 个发现脑氧摄取量增加的解释(174),也是对严重低血压时脑缺氧症状相当明显而没有减少的解释(81)。
Drug-induced forms of coma will be discussed in the following section. In diabetic acidosis and coma a close correlation between reduction of consciousness and of cerebral oxygen uptake was found (169). The finding of increased cerebral blood flow in diabetic coma may be an effect of the severe acidosis (cf. page 204). Severe uremic intoxication with mental symptoms is associated with a reduced cerebral oxygen uptake (139, 276). Uremic anemia is probably the cause of increased cerebral blood flow in some cases (276). In hepatic failure no significant correlation between cerebral depression and oxygen uptake has been found (72, 342). Observations suggesting an increased cerebral ammonia uptake in hepatic coma have been reported (34), but negative or mainly negative studies have since been published (341, 342). It has already been mentioned that in hypoglycemic coma the cerebral perfusion remains normal in spite of a marked reduction of cerebral oxygen uptake (176).
药物引起的昏迷形式将在下一节讨论。在糖尿病性酸中毒和昏迷中,发现意识的减退和脑氧摄取量的减少之间有密切的关系(169)。在糖尿病昏迷中发现脑血流增加可能是严重酸中毒的影响(参见第 204 页)。有精神症状的严重尿毒症中毒与脑氧摄取量减少有关(139,276)。尿毒症贫血可能是某些病例中脑血流量增加的原因(276)。在肝功能衰竭的情况下,没有发现大脑抑郁症和摄氧量之间有明显的相关性(72,342)。已有观察表明肝昏迷时脑氨摄取量增加的报道(34),但此后又有否定的或主要是否定的研究发表(341,342)。已经提到,在低血糖昏迷中,尽管脑氧摄取量明显减少,但脑灌注仍然正常(176)。
Apoplexy. In acute cerebrovascular accidents a distinct correlation between mental and metabolic depression has been reported (199). As the cerebral blood flow is reduced proportionately to the reduction in oxygen metabolism, there seems to be no sign of general cerebral vascular insufficiency in this condition (65, 138, 199). The lack of effect of stellate ganglion block on total cerebral perfusion in apoplexy has been discussed. The inhalation of 100% O2 at atmospheric pressure causes moderate cerebral vasoconstriction in apoplectic patients, just as in normal man (138).
* 在急性脑血管意外中,有报道称精神和代谢抑制之间存在明显的相关性(199)。由于脑血流量的减少与氧代谢的减少成正比,在这种情况下似乎没有一般脑血管功能不全的迹象(65,138,199)。有人讨论过星状神经节阻断对脑瘫患者的全脑灌注缺乏影响。在大气压下吸入 100% 的氧气会使脑瘫患者的脑血管适度收缩,就像在正常人身上一样(138)。
Unilateral carotid ligature was found to be without effect on cerebral blood flow and oxygen uptake in three young subjects who tolerated the operation well; but a 53-year-old man who developed hemiplegia and coma showed reduced values of both flow and oxygen uptake of the brain (303). Bilateral studies, using the original nitrous oxide method, were employed in these observations, which provide an example of the advantage of such techniques when attempting to evaluate the results obtained in the individual subject.
单侧颈动脉结扎被发现对脑血流和摄氧量没有影响,三个年轻的受试者对手术的耐受性很好;但一个 53 岁的男子出现偏瘫和昏迷,显示脑血流和摄氧量的数值都降低了(303)。在这些观察中,采用了最初的氧化亚氮方法进行了双侧研究,这提供了一个例子,说明在试图评估在单个受试者身上获得的结果时,这种技术的优势。
Acute hypertensive encephalopathy is associated with a reduction of cerebral oxygen uptake (206, 228). Whether due to essential hypertension or to the hypertensive toxemia of pregnancy, the cerebral perfusion remains normal in these conditions.
急性高血压脑病与大脑摄氧量的减少有关(206,228)。不管是由于基本高血压还是由于妊娠高血压毒血症,在这些情况下,脑灌注仍然是正常的。
This observation is difficult to evaluate, as no values for the arterial carbon dioxide tensions were reported. It is clear, however, that the cerebral symptoms are not caused by a general insufficiency of cerebral perfusion. Animal experiments have suggested that focal arteriospastic ischemia is the cause of acute hypertensive encephalopathy (45). This concept is not incompatible with the finding of normal cerebral perfusion in patients in hypertensive crisis. Presumably the areas of ischemia are quite small, and thus they contribute little to the over-all perfusion rate. Moreover, if the blood flow in the ischemic zones is sufficiently slow, their contribution would be further minimized.
这一观察结果很难评估,因为没有报告动脉二氧化碳张力的数值。然而,很明显的是,脑部症状不是由普遍的脑灌注不足引起的。动物实验表明,局灶性动脉痉挛性缺血是急性高血压脑病的原因(45)。这一概念与高血压危象患者脑灌注正常的发现并不相悖。据推测,缺血的区域相当小,因此它们对整体的灌注率贡献不大。此外,如果缺血区的血流足够缓慢,它们的贡献就会进一步减弱。
Brain tumor. Kety, Shenkin and Schmidt found a reduced cerebral oxygen uptake and a reduced cerebral perfusion in patients with brain tumor and increased intracranial pressure (175). This observation has been confirmed by several other investigators (25, 30, 118, 120, 121). In the study of Kety and associates, reduced values were found in those patients who had an intracranial pressure higher than about 450 mm H2O. All but one of these patients were comatose. Pressure reduction by ventricular drainage did not cause a rise of the reduced values for cerebral oxygen uptake and cerebral blood flow in these patients, and did not change their level of consciousness (311). This indicates that the high intracranial pressure cannot be the direct cause of the mental, metabolic, and circulatory disturbances of the brain. The high pressure may indirectly be of importance by causing diffuse cerebral damage of a type not immediately reversible following a normalization of the pressure. This damage, e.g. in the form of a cerebral edema or tissue damage caused by the tumor directly, may then be thought of as constituting the more immediate cause of the coma and the reduced cerebral oxygen metabolism. Homeostatic mechanisms and the increased intracranial pressure may both be of importance for the rise in cerebrovascular resistance causing a reduction in cerebral perfusion roughly proportional to the reduction of cerebral oxygen uptake, despite the rise in driving blood pressure.
脑瘤。Kety、Shenkin 和 Schmidt 发现,在患有脑瘤和颅内压增高的病人中,脑氧摄取量减少,脑灌注量降低(175)。这一观察结果已被其他几位研究者证实(25,30,118,120,121)。在 Kety 和同事的研究中,发现那些颅内压高于约 450mmH2O 的病人的数值降低。这些病人中除一人外都是昏迷的。通过心室引流降低压力并没有导致这些病人的脑氧摄取量和脑血流量降低值的上升,也没有改变他们的意识水平(311)。这表明,高颅压不可能是导致大脑精神、代谢和循环障碍的直接原因。高压力可能间接地具有重要意义,因为它造成了弥漫性的脑损伤,而这种损伤在压力正常化后不会立即恢复。这种损害,如脑水肿的形式或由肿瘤直接引起的组织损害,可以被认为是构成昏迷和脑氧代谢减少的更直接原因。静态机制和颅内压升高可能都很重要,尽管驱动血压升高,但脑血管阻力的上升导致脑灌注的减少与脑氧摄取的减少大致成比例。
The cerebral arteriovenous oxygen difference in patients with increased intracranial pressure is normal or slightly increased (25, 30, 52, 109, 118, 120, 121, 175, 311, 345, 351). In normal man, hyperventilation causing mild cerebral symptoms but no reduction of cerebral oxygen uptake markedly increases the cerebral arteriovenous oxygen difference, and the cerebral venous oxygen saturation reaches as low levels as in hypoxia (171). The above mentioned many studies of patients with increased intracranial pressure showed, relative to the changes induced by hyperventilation, a very moderate and probably quite insignificant reduction of cerebral venous oxygen saturation. Thus there is no convincing evidence of a diffuse cerebral circulatory derangement causing a generalized cerebral hypoxia.
颅内压升高的病人的脑动静脉氧差正常或略有增加(25, 30, 52, 109, 118, 120, 121, 175, 311, 345, 351)。在正常人中,引起轻度脑部症状但不减少脑氧摄取量的过度通气会明显增加脑动静脉氧差,而脑静脉氧饱和度达到与缺氧时一样低的水平(171)。上述许多对颅内压增高病人的研究显示,相对于过度通气引起的变化,脑静脉氧饱和度的降低非常适度,可能相当不明显。因此,没有令人信服的证据表明,弥漫性脑循环失调会导致普遍的脑缺氧。
Extraneous influences have been studied to some extent. Pressure reduction by ventricular drainage has, as mentioned above, no effect (311). The intravenous administration of hypertonic glucose was found to reduce the increased pressure in some cases without changing the clinical condition or changing the subnormal value for cerebral oxygen uptake (311). Moderate hypotension induced by a ganglionic blocking agent was found not to change the cerebral perfusion or oxygen uptake in patients with moderately increased intracranial pressure (24). This observation indicates that the cerebral circulation is not on the verge of collapse, and that induced hypotension may presumably be used safely during operation in such patients. In a small series of cases, tilting 200 head up was found to decrease the cerebral blood flow in patients with brain tumor, whereas tilting 200 head down had no significant effect (310).
外界的影响因素在一定程度上已被研究。如上所述,通过心室引流降低压力没有效果(311)。发现静脉注射高渗葡萄糖可以降低某些病例的压力升高,但不改变临床状况,也不改变脑氧摄取量的异常值(311)。发现由神经节阻断剂诱导的中度低血压不会改变中度颅内压升高患者的脑灌注或摄氧量(24)。这一观察表明,脑循环没有处于崩溃的边缘,诱导性低血压大概可以在这类病人的手术中安全使用。在一个小系列的病例中,发现将 200 头向上倾斜会减少脑瘤患者的脑血流量,而将 200 头向下倾斜则没有明显的影响(310)。
# 器质性疾呆
Organic Dementia
The cerebral oxygen uptake is subnormal in chronic diffuse organic brain diseases characterized by a reduction of intellectual mental functions. This was first reported by Freyhan, Woodford and Kety in a study of senile brain disorders (96). It has been confirmed since by studies of other chronic brain disorders, such as cerebral syphilis (251), or chronic brain syndrome following acute cerebrovascular accidents (31, 63, 66, 70, 179, 180, 190, 241, 248, 309).
慢性弥漫性有机脑病的脑氧摄取量不正常,其特点是智力精神功能下降。这是 Freyhan、Woodford 和 Kety 在对老年性脑病的研究中首次报道的(96)。此后,对其他慢性脑病的研究也证实了这一点,如脑梅毒(251),或急性脑血管意外后的慢性脑综合症(31,63,66,70,179,180,190,241,248,309)。
A definite relation between the degree of reduction of cerebral oxygen uptake and the degree of dementia was found by Garfunkel, Baird and Ziegler (100), who studied mentally retarded children with various severe neurological diseases. The same observation was made in a study of aged patients with degenerative brain diseases of different etiology studied by Lassen, Munck and Tottey (190). The latter results were obtained by employing bilateral studies using the Kr83 technique, an approach which was found greatly to facilitate this correlation. The results of these studies may be summarized as follows: In patients whose mental condition is completely dominated by severe loss of intelligence, the cerebral oxygen uptake is reduced to about 2.0 cc per 100 gm per minute, while in those with less apparent dementia the values lie between 2.5 and 3.0.
Garfunkel、Baird 和 Ziegler(100)研究了患有各种严重神经系统疾病的弱智儿童,发现脑氧摄取量的减少程度与痴呆程度之间有明确的关系。Lassen、Munck 和 Tottey(190)对患有不同病因的退行性脑病的老年患者进行了研究,也有同样的观察结果。后者的结果是通过使用 Kr83 技术的双侧研究获得的,这种方法被认为大大促进了这种相关性。这些研究的结果可归纳如下。在精神状况完全被严重的智力丧失所支配的病人中,脑氧摄取量减少到每 100 克 / 分钟约 2.0 毫升,而在那些痴呆不太明显的病人中,其数值在 2.5 和 3.0 之间。
Severe organic dementia is associated with the same low values of cerebral oxygen uptake per 100 grams of brain per minute as were found in coma.6 These two conditions are, however, clinically strikingly different. Subjects with such degrees of organic dementia have no loss of consciousness. Although severely incapacitated socially by loss of intellectual faculties and by some degree of emotional fatuity or instability, such patients are often able to care for personal requirements and, given proper care, to remain in their home environment (190). Possibly the gradual but complete loss of many cortical cells does not affect cortical function as profoundly as the severe hypofunction of all cortical cells supposedly found in coma. It is also possible that in coma the loss of consciousness and reduction of cortical oxygen uptake are both secondary to the depression of subcortical centers, which remain intact in chronic brain disease (see e.g. 215).
严重的器质性痴呆与昏迷时每 100 克脑的摄氧量的低值相同 6。患有这种程度的器质性痴呆的人没有意识丧失。尽管由于智力丧失和某种程度的情感疲劳或不稳定而严重丧失了社会能力,但这些病人往往能够满足个人需求,并且在适当的照顾下,能够留在他们的家庭环境中(190)。可能许多皮质细胞的逐渐但完全丧失对皮质功能的影响并不像据称在昏迷中发现的所有皮质细胞的严重功能低下那样深远。也有可能在昏迷中,意识的丧失和皮层摄氧量的减少都是继发于皮层下中心的抑制,而这些中心在慢性脑病中仍然保持完整(见例如 215)。
Organic dementia of known etiology. It is well established that cerebral oxygen uptake and cerebral blood flow are reduced in patients who develop chronic brain syndrome following an acute cerebrovascular accident (31, 63, 66, 70, 138, 179, 180, 190, 241, 248, 309). Cases with proven thrombosis of the internal carotid artery have the same abnormalities of cerebral circulation and metabolism (245).
* 已知病因的器质性痴呆。* 在急性脑血管意外后发生慢性脑综合征的病人中,脑氧摄取量和脑血流量减少是公认的(31, 63, 66, 70, 138, 179, 180, 190, 241, 248, 309)。经证实的颈内动脉血栓形成的病例也有同样的脑循环和代谢的异常(245)。
8 Presumably the oxygen uptake for the total brain is actually lower in such cases of severe chronic brain disease than it is in coma, as only in the former condition is loss of cerebral tissue supposedly quantitatively important.
8 据推测,在这种严重的慢性脑病病例中,全脑的摄氧量实际上比昏迷时要低,因为只有在前一种情况下,脑组织的损失才应该是定量的。
Cerebral oxygen uptake and cerebral perfusion were also found to be reduced in meningovascular lues and in dementia paralytica, whereas normal values were found in asymptomatic neurolues (251). Thus in this condition also a clear correlation between decreased cerebral function and reduced cerebral oxygen uptake could be demonstrated. Clinical improvement in patients with dementia paralytica treated with penicillin or penicillin combined with pyrogen caused an increase of cerebral oxygen uptake towards the normal level (251). In acute experiments, pyrogen therapy (to 39 °C) was found to cause only minor changes in asymptomatic cases, but to increase cerebral perfusion and oxygen uptake significantly in patients with dementia paralytica (140). This observation is not easy to interpret. The results reported are not incompatible with the hypothesis that the hyperthermia had in actual fact caused a 10-15 per cent increase in cerebral oxygen uptake in both groups, as was mentioned previously. Children with congenital neurological disorders have been found to have reduced values for cerebral oxygen uptake and cerebral blood flow (100). The reduction of the cerebral metabolic rate of oxygen showed a clear correlation to the degree of retardation of intellectual development. In a study of four patients with microcephalia and a very low level of intelligence, moderately subnormal values for cerebral oxygen metabolism and perfusion were found (78). In such patients, however, where the weight of the brain is so much lower than normal, total cerebral oxygen uptake and perfusion is consequently markedly reduced. A reduction of cerebral oxygen uptake and cerebral perfusion has been reported in advanced cases of chronic encephalitis (314). Bilateral stellectomy in these patients caused no significant changes.
在脑膜血管病和瘫痪性痴呆中也发现脑氧摄取量和脑灌注量减少,而在无症状的神经病变中则发现正常值(251)。因此,在这种情况下,也可以证明脑功能下降和脑氧摄取量减少之间有明显的相关性。用青霉素或青霉素结合热原治疗瘫痪性痴呆患者的临床症状得到改善,使脑氧摄取量增加,达到正常水平(251)。在急性实验中,发现热原治疗(至 39℃)在无症状的病例中只引起轻微的变化,但在痴呆瘫痪的病人中却能明显增加脑灌注和氧摄取量(140)。这一观察结果不容易解释。所报告的结果与之前提到的假设并不冲突,即热疗实际上导致两组患者的脑氧摄取量增加了 10-15%。已发现患有先天性神经系统疾病的儿童的脑氧摄取量和脑血流量的数值降低(100)。大脑氧气代谢率的降低与智力发育迟缓的程度显示出明显的相关性。在一项对四名患有小儿麻痹症和智力水平很低的病人的研究中,发现脑氧代谢和灌注的数值中等偏下(78)。然而,在这样的病人中,大脑的重量比正常人低得多,总的脑氧摄取和灌注也因此而明显减少。在慢性脑炎的晚期病例中,也有脑氧摄取量和脑灌注量减少的报道(314)。这些病人的双侧支架切除术没有引起明显的变化。
# 大脑动脉硬化
Cerebral Arteriosclerosis
Chronic brain disease with organic dementia is common in the older age groups. Such patients are clinically characterized by a reduction of intellectual functions which often socially incapacitates the individual. In all the many studies of such patients which will be referred to in this section, the cerebral oxygen uptake is subnormal and seems roughly to correlate with the reduction of mental powers. Chronic organic brain disease in elderly people is in some cases caused by well defined cerebral diseases, such as cerebral syphilis or acute cerebrovascular accidents. These disorders have been discussed in the previous section. In a great many cases, however, the development of chronic brain syndrome is very gradual, and its cause remains obscure. It is common to use the term ‘cerebral arteriosclerosis’ to describe such cases. This term expresses the opinion that progressive atheromatous narrowing of the cerebral arteries is the cause of diffuse, slowly progressive cerebral atrophy. If hypertension, retinopathy, stenocardia, or other signs of vascular disease are present, they are taken to constitute supportive evidence for the assumption of a vascular etiology.
患有器质性痴呆的慢性脑病在老年人群中很常见。这类病人的临床特点是智力功能下降,常常使个人丧失社会能力。在本节将提到的对这类病人的所有研究中,脑氧摄取量是不正常的,而且似乎与智力下降大致相关。老年人的慢性器质性脑病在某些情况下是由明确的脑部疾病引起的,如脑梅毒或急性脑血管意外。这些疾病已经在上一节中讨论过了。然而,在许多情况下,慢性脑综合征的发展是非常渐进的,而且其原因仍然不明确。人们通常用 "脑动脉硬化" 一词来描述这种情况。这个术语表达了这样的观点:脑动脉的渐进性粥样硬化狭窄是造成弥漫性、缓慢进行的脑萎缩的原因。如果存在高血压、视网膜病变、心肌梗塞或其他血管疾病的迹象,它们被认为构成了血管病因假设的支持性证据。
The syndrome just described is clinically related to that of various forms of supposedly nonvascular progressive cerebral atrophy affecting the same age groups. Alzheimer’s and Pick’s diseases are among the more well defined and recognizable of these disorders, which presumably primarily affect the parenchyma of the brain. How can one distinguish clinically between primary atrophy of the cerebral parenchyma and cellular damage secondary to cerebral vascular disease? With the advent of methods which allow measurement of cerebral blood flow and other important cerebral circulatory parameters in such patients, it was to be hoped that this distinction could be made more clearly. As will become apparent in the following, this has not been the case.
刚刚描述的综合征在临床上与影响同一年龄组的各种形式的所谓非血管性进行性脑萎缩有关。阿尔茨海默氏症和皮克氏症是这些疾病中定义更明确、更易识别的疾病,据推测它们主要影响脑实质。如何在临床上区分脑实质的原发性萎缩和继发于脑血管疾病的细胞损伤?随着能够测量这类病人的脑血流和其他重要的脑循环参数的方法的出现,人们希望能够更清楚地作出这种区分。正如下文所显示的,情况并非如此。
Cerebral circulation in cerebral arteriosclerosis. A high incidence of severe atheromatosis of the larger cerebral arteries is generally found in elderly patients who die from acute cerebrovascular accidents. This observation has led to the probably correct assumption that elderly patients surviving an apoplectic insult have, as a group, a more pronounced degree of cerebral atheromatosis than nonapoplectic controls of the same age or normal young adults. On this basis, information regarding the cerebral circulation in ‘cerebral arteriosclerosis’ has in most cases been deduced from studies of aged post-apoplectic cases and suitable controls.
* 在因急性脑血管意外死亡的老年患者中,一般会发现较大的脑动脉严重粥样硬化的高发率。这一观察结果导致了一个可能是正确的假设,即老年患者在受到天旋地转的伤害后,作为一个群体,比同龄的非天旋地转的对照组或正常的年轻人有更明显的脑动脉粥样硬化程度。在此基础上,有关 "脑动脉硬化" 的脑循环信息在大多数情况下都是通过对老年折返病患者和合适的对照组的研究推导出来的。
A normal level of oxygen saturation of the cerebral venous blood is found in postapoplectic patients (63, 66, 138, 289, 309; see also 44 and 315, in which the clinical material was somewhat differently selected). Assuming the gradient of oxygen tension between the brain and the cerebral venous blood is not markedly increased, it must be concluded that the over-all oxygen tension of the brain is maintained at an adequate level in aged patients who have survived a stroke. This important conclusion is supported by the observation that hyperventilation or induced hypotension may reduce the cerebral perfusion and the cerebral venous oxygen tension in such patients below the resting level without causing symptoms of diffuse cerebral hypoxia (31, 66, 179, 180).
大脑静脉血的氧饱和度在瘫痪后的病人中是正常的(63,66,138,289,309;也见 44 和 315,其中的临床材料选择有些不同)。假设大脑和脑静脉血之间的氧张力梯度没有明显增加,就必须得出结论,在中风后幸存的老年患者中,大脑的整体氧张力保持在一个足够的水平。这一重要结论得到了以下观察的支持:过度通气或诱导性低血压可使这些病人的脑灌注和脑静脉血氧张力降低到静止水平以下,而不会引起弥漫性脑缺氧的症状(31, 66, 179, 180)。
Focal cerebral vascular insufficiency is, however, not excluded from these observations. It is clinically well established that marked hypotension in elderly patients may occasionally lead to localized cerebral ischemia or even infarction, presumably because of a local inadequacy of the compensatory vasodilatation (51, 56, 70). Supposedly this syndrome is caused by the preexistence of an occlusion or marked narrowing of a larger cerebral artery. In response to such a pathological obstruction, the collateral vessels to the area are already dilated so much that the further vasodilatation in response to hypotension is inadequate (220).
然而,这些观察结果并不排除局域性脑血管功能不全的可能。临床上已经证实,老年患者的明显低血压偶尔会导致局部脑缺血甚至梗死,这可能是因为局部补偿性血管舒张不足(51,56,70)。据推测,这种综合征是由预先存在的较大的脑动脉的闭塞或明显狭窄引起的。在应对这种病理性阻塞时,该区域的侧支血管已经扩张得很厉害,以至于对低血压的进一步血管扩张是不够的(220)。
If focal cerebral hypofunction during induced hypotension were to be taken as the only reliable clinical evidence of significant cerebral vascular disease, then this diagnosis would be a rare one, as it is well recognized that this syndrome is not common (5). In this connection it is relevant to report the results of Fazekas’ and co-workers’ study of the effect of induced hypotension in 12 elderly hypertensive patients, all with signs of chronic brain disease and presumed cerebral atheromatosis (70). When the blood pressure was reduced to half the control value, these patients developed signs of diffuse cerebral hypoxia. No signs of focal cerebral hypoxia were found. These results are completely comparable to those obtained in younger hypertensive patients without signs of cerebral disease (168). Undoubtedly many if not all of the elderly patients studied by Fazekas and co-workers had atheromatosis of their cerebral arteries. Despite this, no focal or general cerebral vascular insufficiency was disclosed by the induced hypotension.
如果把诱导性低血压期间的局灶性脑功能低下作为明显的脑血管疾病的唯一可靠的临床证据,那么这种诊断将是一种罕见的诊断,因为大家都知道这种综合征并不常见(5)。在这方面,有必要报告 Fazekas 和他的同事对 12 名老年高血压患者的诱导性低血压的影响的研究结果,这些患者都有慢性脑部疾病的症状,并假定有脑动脉粥样硬化(70)。当血压降低到控制值的一半时,这些病人出现了弥漫性脑缺氧的症状。没有发现局灶性脑缺氧的迹象。这些结果与在没有脑部疾病迹象的年轻高血压患者身上得到的结果完全相当(168)。毫无疑问,Fazekas 和他的同事所研究的老年患者中,即使不是全部,也有许多人的脑动脉有粥样硬化。尽管如此,在诱导性低血压中没有发现局灶性或全身性的脑血管功能不全。
Carbon dioxide inhalation causes cerebral vasodilatation in elderly patients who have survived stroke (63, 66, 241, 248, 289). A detailed evaluation of these studies is difficult, as the values for the arterial pCO2 have not been reported, but the average percentage increase in cerebral blood flow is the same as found in normal young adults. Fazekas and co-workers found no increase in cerebral perfusion in a few of their old patients (66). This interesting observation remains isolated, however, as no other studies have reported similar cases (63, 190, 241, 248, 289).
在中风后幸存的老年患者中,吸入二氧化碳会引起脑血管扩张(63, 66, 241, 248, 289)。对这些研究的详细评估是困难的,因为没有报告动脉 pCO2 的值,但脑血流的平均增加百分比与在正常年轻人中发现的相同。Fazekas 和他的同事发现在他们的几个老年患者中,脑灌注没有增加(66)。然而这一有趣的观察仍然是孤立的,因为没有其他研究报告类似的情况(63,190,241,248,289)。
It is necessary to discuss two of the above mentioned studies further, as the authors did not draw the same conclusions from their observations as has the present reviewer. Novak and collaborators found that carbon dioxide did not significantly decrease the cerebrovascular resistance in a group of normotensive postapoplectic patients (241). The data reported suggest, however, that this observation was caused by random errors. Let it be assumed that the calculated cerebral oxygen uptake had remained constant in each case of this group (as it is well known that carbon dioxide does not affect the cerebral oxygen uptake (174)). Then it can be calculated that the cerebrovascular resistance actually did decrease significantly in this group just as in the other groups studied.
有必要进一步讨论上述研究中的两项,因为作者并没有像本评论员一样从他们的观察中得出相同的结论。诺瓦克和合作者发现,在一组血压正常的抽搐后患者中,二氧化碳并没有明显降低脑血管阻力(241)。然而,报告的数据表明,这一观察是由随机误差引起的。让我们假设在该组的每个病例中,计算出的脑氧摄取量保持不变(因为众所周知,二氧化碳不影响脑氧摄取量(174))。然后可以计算出,在这一组中,脑血管阻力实际上确实明显下降,就像在其他研究组一样。
Schieve and Wilson found that the increase of cerebral perfusion during carbon dioxide inhalation was lower in elderly patients with organic brain syndrome than in normals (289). But these authors failed to take into consideration the fact that the carbon dioxide reactivity depends on the initial value for the cerebral blood flow. This relation was clearly apparent from a study of the carbon dioxide reactivity of anesthetized normal subjects which were studied by the same authors (289). The relative increase in cerebral blood flow during carbon dioxide administration was found to be approximately the same in chronic brain disease and anesthesia as in normal man. This means that the induced changes of the carbon dioxide and the oxygen tensions of the cerebral venous blood is the same in all three groups. Thus it seems permissible to conclude that the results obtained by Schieve and Wilson demonstrated an adequate carbon dioxide reactivity in patients with organic brain disease.
Schieve 和 Wilson 发现,在吸入二氧化碳时,老年有机脑综合征患者的脑灌注量的增加低于正常人(289)。但是这些作者没有考虑到一个事实,即二氧化碳的反应性取决于脑血流量的初始值。这种关系在同一作者对麻醉的正常人的二氧化碳反应性的研究中是很明显的(289)。发现在慢性脑病和麻醉状态下,脑血流的相对增加与正常人大致相同。这意味着,在所有三组中,诱发的二氧化碳和脑静脉血氧张力的变化是相同的。因此,似乎可以得出这样的结论:Schieve 和 Wilson 获得的结果表明,有机脑病患者有足够的二氧化碳反应性。
It thus seems that the regulation of the cerebral blood flow is relatively normal in the average old patient who has survived a stroke; the changes of cerebral perfusion induced by hypotension, hyperventilation and carbon dioxide have already been reviewed. Alterations in the inspired oxygen concentration (63, 138) and aminophylline injections (66) also change the cerebral perfusion in elderly postapoplectic patients as in normal man.
这样看来,在中风后幸存的普通老年患者中,脑血流的调节是相对正常的;由低血压、过度通气和二氧化碳引起的脑灌注的变化已被回顾。氧气浓度的改变(63,138)和氨茶碱注射(66)也会改变老年脑卒中后病人的脑灌注,就像正常人一样。
The following two statements find support in the many studies reviewed in this section: z) Atheromatosis of the cerebral arteries usually does not cause progressive narrowing of vessels of functional importance. This has also been demonstrated directly by pathoanatomical observations of the diameter of atheromatous cerebral arteries (37). 2) The vessels regulating the cerebrovascular resistance are not abnormally rigid in patients who have atheromatosis of the cerebral arteries. This statement is likewise supported by independent evidence, as atheromatosis of the cerebral arteries is confined to arteries of a diameter of more than 0.2 mm (3), whereas the cerebrovascular resistance is presumably mainly regulated by even smaller arteries (82).
以下两种说法在本节回顾的许多研究中得到了支持: z) 脑动脉粥样硬化通常不会导致具有重要功能的血管逐渐狭窄。对动脉粥样硬化的脑动脉直径的病理观察也直接证明了这一点(37)。2) 在脑动脉粥样硬化的病人中,调节脑血管阻力的血管并没有异常的僵硬。这一说法同样得到了独立证据的支持,因为脑动脉粥样硬化仅限于直径超过 0.2 毫米的动脉(3),而脑血管阻力可能主要由更小的动脉调节(82)。
Chronic brain disease and cerebral arteriosclerosis; conclusion. The measurement of total cerebral perfusion or the cerebral venous oxygen tension cannot, in the average case, disclose the presence of atheromatosis of the cerebral arteries, not even when studies are made during induced hypotension or carbon dioxide inhalation. Thus it is not possible by using such techniques to divide the many presenile and senile patients into two groups, one of vascular etiology and one of nonvascular etiology. This negative conclusion is, however, not the only one which can be derived from the many studies reviewed above. The adequacy of the oxygen delivery of the brain and of the regulation of cerebral blood flow in patients with atheromatosis of the cerebral arteries deserves some further comments. On this basis one may question whether a gradual atheromatous narrowing of the larger cerebral arteries is actually a common cause of progressive presenile and senile chronic brain disease. The studies of the cerebral circulation in elderly patients thus deemphasize the pathogenetic importance of cerebral atheromatosis in chronic progressive brain disease in the higher age groups. The possibility of primary parenchymatous processes must be considered in all such patients regardless of circumstantial evidence of atheromatosis of the cerebral vessels.
* 慢性脑病和脑动脉硬化;结论。* 在一般情况下,测量全脑灌注量或脑静脉氧张力不能揭示脑动脉粥样硬化的存在,即使在诱导性低血压或吸入二氧化碳时进行研究也不行。因此,利用这些技术不可能将许多先天性和老年性患者分成两组,一组是血管病因,一组是非血管病因的。然而,这个否定的结论并不是从上述许多研究中可以得出的唯一结论。脑动脉粥样硬化患者的脑供氧和脑血流调节是否充分,值得进一步评论。在此基础上,人们可能会质疑较大的脑动脉的逐渐粥样变窄是否真的是渐进性的老年性慢性脑病的一个共同原因。因此,对老年患者脑循环的研究不再强调脑动脉粥样硬化在高年龄组慢性进行性脑病中的致病重要性。无论是否有脑血管粥样硬化的间接证据,都必须考虑所有这类患者的原发性实质过程的可能性。
# 老年患者的慢性脑病和精神病
Chronic Brain Disease and Psychoses in Aged Patients
Frey han and collaborators (96) studied a group of ten aged patients (average age 72 years) who were institutionalized because of gross mental defects of psychotic proportion (confusion, pronounced loss of recent memory, severe emotional lability etc.). These patients had moderately lower values for the cerebral perfusion and oxygen uptake than normal young adults studied by the same group of investigators. The subnormal cerebral oxygen consumption may be taken to indicate diffuse chronic organic brain disease in the group of aged psychotic patients as a whole.
Frey han 及其合作者(96)研究了一组 10 名老年患者(平均年龄 72 岁),他们因严重的精神缺陷(意识混乱、明显丧失近期记忆、严重的情绪不稳定等)而被送入精神病院。这些病人的脑灌注和摄氧量的数值比同一组调查人员研究的正常年轻人要低。大脑耗氧量的不正常可以被认为是表明在整个老年精神病患者群体中弥漫性的慢性有机脑病。
Nonpsychotic aged subjects with no obvious signs of disease have been found to have a similar reduction of the cerebral metabolic rate of oxygen (63, 279, 289), while very highly selected, optimally normal old subjects showed no demonstrable reduction (320). These observations, which have already been discussed in the section on the influence of age, may be interpreted to indicate that many elderly nonpsychotic subjects have a reduced cerebral oxygen uptake on the basis of chronic brain disease. Thus it seems that with regard to diffuse organic brain disease as evidenced by a decreased cerebral oxygen uptake, psychotic old patients are not more severely affected than many alert, sane persons of the same age. In the latter cases the clinical signs of cerebral hypofunction are restricted to an inconspicuous reduction of intellectual abilities. The study of Fazekas and associates on the cerebral circulation and oxygen uptake in elderly patients seems to support this hypothesis (63, 68). The authors failed to find any significant difference of cerebral oxygen metabolism between ‘alert’ and ‘confused’ aged patients. The cerebral oxygen uptake was reduced to the same extent in both groups.
没有明显疾病迹象的非精神病老年受试者也被发现有类似的脑氧代谢率的降低(63,279,289),而经过高度筛选的、最正常的老年受试者没有显示出明显的降低(320)。这些观察结果已经在关于年龄影响的章节中讨论过了,可以解释为许多非精神病患者的老年受试者在慢性脑部疾病的基础上有脑氧摄取量的降低。这样看来,在以脑摄氧量下降为证据的弥漫性脑部疾病方面,老年精神病患者并不比许多同龄的警觉、理智的人受到更严重的影响。在后一种情况下,脑功能低下的临床表现仅限于智力的不明显下降。Fazekas 和他的同事对老年患者的脑循环和摄氧量的研究似乎支持这一假设(63,68)。作者没有发现 "警觉的" 和 "困惑的" 老年患者之间的脑氧代谢有任何明显的差异。两组患者的脑氧摄取量都有相同程度的减少。
Thus, in psychosis developing in aged patients, just as in schizophrenic psychosis, the derangement of cerebral function does not correlate with the cerebral oxygen uptake. The clinical syndrome of psychotic behavior in old patients is usually described by the terms ‘senile psychosis’ or ‘organic psychosis.’ Both terms imply an intimate connection between organic (and presumably irreversible) brain lesions and the abnormal behavior. The studies mentioned above suggest that these concepts may be too simple. They do suggest that psychotic behavior in old people more frequently develops in the presence of chronic organic cerebral disease, but they do not indicate a close relation between the severity of diffuse organic brain disease and the degree of psychiatric disturbance.
因此,在老年患者的精神病中,就像在精神分裂症的精神病中一样,脑功能的失调与脑氧摄取量没有关系。老年患者的精神病行为的临床综合征通常用 "老年性精神病" 或 "器质性精神病" 来描述。这两个术语都意味着有机的(而且可能是不可逆的)脑部病变与异常行为之间存在密切的联系。上述研究表明,这些概念可能过于简单。它们确实表明,老年人的精神病行为更多地是在存在慢性器质性脑病的情况下发生的,但它们并没有表明弥漫性器质性脑病的严重程度与精神障碍的程度之间有密切的关系。
# 其他神经精神疾病
Miscellaneous Neuropsychiatric Disorders
Grant and co-workers found in patients with idiopathic epilepsy that when no seizure occurs during the actual study, the cerebral oxygen uptake and blood flow are normal (116). This has also been reported by Gibbs and associates, employing the indicator injection method (104). (This is the only study, so far, in which the indicator injection method was used to study a distinct disease entity.) No change of cerebral blood flow occurs immediately preceding a seizure (109). Studies in monkeys during induced epileptiform attacks have demonstrated that cerebral oxygen uptake and perfusion increase to about twice the control value (294). Direct observations in man by Penfield have suggested a local increase of perfusion through that portion of the cortex which is involved in the convulsive discharge (254). As mentioned previously, it is possible that during spontaneous seizures in man, arterial hypoxia may interfere seriously with the cerebral oxygen delivery. Patients who are semicomatose immediately following induced seizures have been found to have subnormal values for cerebral oxygen uptake and cerebral perfusion (116, 176). The effects of repeated electric shock therapy have been studied on a group of 21 psychotic patients without evidence of organic brain disease (347). Following a series of, in average, 10 electroshock treatments, no significant change in cerebral oxygen uptake or cerebral blood flow could be demonstrated.
格兰特和同事在特发性癫痫患者中发现,当实际研究期间没有发作时,脑氧摄取量和血流量是正常的(116)。吉布斯和同事也报告了这一点,他们采用了指标注射法(104)。(这是迄今为止唯一的一项研究,在这项研究中,指标注射法被用来研究一种独特的疾病实体。) 癫痫发作前没有发生脑血流的变化(109)。在诱导癫痫发作期间对猴子的研究表明,脑氧摄取和灌注增加到控制值的两倍左右(294)。潘菲尔德对人的直接观察表明,参与抽搐放电的那部分大脑皮层的局部灌注增加(254)。如前所述,在人的自发性癫痫发作期间,动脉缺氧可能会严重干扰脑部氧气的输送。已经发现在诱导癫痫发作后立即处于半瘫痪状态的病人,其脑氧摄取和脑灌注的数值都不正常(116,176)。有人对一组没有脑部器质性疾病证据的 21 名精神病患者研究了反复电击疗法的影响(347)。经过一系列平均 10 次的电击治疗,可以证明脑氧摄取量或脑血流没有明显的变化。
Disseminated sclerosis. Reduced values for cerebral oxygen uptake and cerebral blood flow have also been reported in this disease (114, 277, 338). Due to the large scatter of values obtained in the pathological groups and in the control groups, these reductions were not statistically significant. The fact that in all three clinical studies distinctly subnormal average values were reported does, however, suggest that the cerebral oxygen uptake and perfusion actually are reduced in severe cases of this disease.
* 在这种疾病中也有脑氧摄取量和脑血流量降低的报道(114,277,338)。由于在病理组和对照组中获得的数值有很大的分散性,这些降低的数值在统计学上没有意义。然而,在所有三项临床研究中都报告了明显低于正常的平均值,这一事实表明,在这种疾病的严重病例中,脑氧摄取和灌注实际上是下降的。
Lobotomy. Following lobotomy cerebral oxygen uptake and cerebral blood flow have been found to be reduced (313). The authors suggest as one possible explanation, that the disruption of association neurones decreases the total number of stimuli and thus the total number of discharges from the brain—thereby reducing the cerebral oxygen uptake and accordingly the cerebral blood flow also.
* 脑叶切除术后,脑氧摄取量和脑血流量被发现减少(313)。作者提出一个可能的解释,即联想神经元的中断减少了刺激的总数,从而减少了大脑放电的总数,从而减少了脑氧摄取量,也相应减少了脑血流量。
Intracranial arteriovenous aneurisms. Cerebral blood flow is markedly increased in this condition, while the cerebral oxygen uptake is maintained at the normal level. In spite of unilateral localization of the shunt, some patients have high values for the calculated cerebral blood flow per 100 gm of tissue in both internal jugular veins, whereas others have high values predominantly on the affected side (26, 28, 33, 189, 286, 312). It has been estimated that the smallest shunt which can be demonstrated using the Kr85 modification is about 200 cc per minute (189).
* 颅内动静脉瘤。* 在这种情况下,脑血流量明显增加,而脑氧摄取量则维持在正常水平。尽管分流的位置是单侧的,但有些病人在两条颈内静脉中每 100 克组织的计算脑血流值很高,而有些病人的高值主要在受影响的一侧(26,28,33,189,286,312)。据估计,用 Kr85 修改法能显示的最小分流值约为每分钟 200 毫升(189)。
Schizophrenia. A large series of chronic schizophrenic patients studied by Kety and co-workers (176) showed completely normal values for cerebral oxygen uptake and cerebral perfusion. Wilson and his collaborators (347) and Sokoloff et al. (322) have reported similar findings. Moderately subnormal values were reported by Gordan and co-workers (114). It is difficult to explain these divergent results, as the case materials studied and the experimental techniques used seem to have been quite similar in all studies. On the basis of the four studies mentioned, however, it is unlikely that chronic schizophrenic patients have a significant impairment of total cerebral perfusion and oxygen metabolism.
*Kety 和他的同事(176)研究的一大批慢性精神分裂症患者显示,脑氧摄取量和脑灌注量的数值完全正常。Wilson 和他的合作者(347)以及 Sokoloff et al.(322)也报告了类似的结果。Gordan 和合作者(114)报告了中等程度的亚正常值。很难解释这些不同的结果,因为所有研究中所研究的病例材料和所使用的实验技术似乎都很相似。然而,根据上述四项研究,慢性精神分裂症患者不太可能有总脑灌注和氧代谢的明显损害。
The finding of a fairly normal cerebral oxygen uptake in schizophrenia is interesting. A marked reduction of intellectual performance is not rare in such patients. This dementia, however, is apparently quite different from the dementia found in degenerative brain diseases, where the mental and metabolic functions of the brain are both reduced. These observations support the widely accepted view that when dementia occurs in schizophrenics, it is secondary to the more fundamental derangement of affective cerebral functions. The lack of obvious changes in gross energy requirement of the brain in schizophrenia may be commented on by using Kety’s words regarding the lack of correlation between cerebral oxygen uptake and cerebral dysfunction in hypoxia and hyperventilation (174): “The higher psychic functions are associated with biochemical changes so subtle and complex as to render any attempt to describe them in terms of mere oxygen utilization no more adequate than to predict the fidelity of a radio by its power requirements.”
发现精神分裂症患者的脑氧摄取量相当正常,这很有意思。在这类病人中,智力表现明显下降的情况并不罕见。然而,这种痴呆显然与退行性脑病中发现的痴呆完全不同,在退行性脑病中,大脑的精神和代谢功能都会降低。这些观察结果支持了一个被广泛接受的观点,即当精神分裂症患者发生痴呆时,它是继发于情感性脑功能的更基本的失调。在精神分裂症中,大脑的总能量需求缺乏明显的变化,可以用 Kety 关于在缺氧和过度换气时脑氧摄取量和脑功能障碍之间缺乏相关性的话来评论(174)。"高级精神功能与生化变化有关,这些变化是如此微妙和复杂,以至于使任何试图用单纯的氧气利用来描述它们的做法都不充分,就像用功率要求来预测收音机的保真度一样"。
# 各类系统性疾病
Various Systemic Disorders
Hypotension. Patients with spontaneous orthostatic hypotension were studied by Finnerty and co-workers (81). A reduction of the mean arterial blood pressure at head level induced by tilting was found to cause clinical symptoms of inadequate cerebral perfusion when the pressure was reduced to about 40-50 per cent of the control level. Concomitantly the cerebral blood flow was reduced to a critical level of about 60 per cent of the control value, while the cerebral oxygen uptake was not significantly reduced. This response is typical for all forms of severe hypotension, whether induced by changes of posture in susceptible patients (81), by spinal anesthesia (159, 184, 185), or by various drugs (81, 229, 230). In moderate hypotension, adequate dilatation of the cerebral vessels occurs, maintaining cerebral blood flow at the normal level (1, 23, 49, 58, 124, 125, 130, 179, 278).
*Finnerty 和他的同事研究了自发性直立性低血压的病人(81)。通过倾斜引起的头部平均动脉血压的降低,发现当压力降低到控制水平的 40-50% 时,会引起脑灌注不足的临床症状。同时,脑血流量减少到控制值的 60% 左右的临界水平,而脑氧摄取量没有明显减少。这种反应在所有形式的严重低血压中都很典型,无论是由易感病人的姿势改变(81)、脊髓麻醉(159,184,185),还是由各种药物(81,229,230)引起的。在中度低血压中,脑血管发生充分扩张,将脑血流维持在正常水平(1, 23, 49, 58, 124, 125, 130, 179, 278)。
::::
Studies in acute hemorrhagic shock have demonstrated a pronounced reduction of arterial pCO2 due to hyperventilation (331). This was presumably the cause of the reduction of cerebral blood flow to levels lower than could be explained by the hypotension per se. A small dose of morphine sulphate caused a rise in arterial pCO2 towards normal values and a normalization of the cerebral blood flow without any change in blood pressure. The subjective state of the patients was also considerably improved by the drug. Subnormal values for cerebral blood flow and oxygen uptake have been reported in secondary shock of varying etiology (69). Owing to the heterogeneity of the material and the paucity of the clinical information it is difficult to interpret these results.
对急性失血性休克的研究表明,由于过度通气,动脉 pCO2 明显减少(331)。这可能是导致脑血流减少到低于低血压本身所能解释的水平的原因。小剂量的硫酸吗啡使动脉 pCO2 上升到正常值,并使脑血流正常化,而血压没有任何变化。患者的主观状态也因该药物而得到了很大的改善。在不同病因的继发性休克中都有脑血流和摄氧量低于正常值的报道(69)。由于材料的异质性和临床资料的匮乏,很难解释这些结果。
Essential hypertension. Cerebral blood flow and oxygen uptake are normal in patients with essential hypertension without cerebral complications (122, 166, 172). This means that cerebrovascular resistance is increased in proportion to the increase in mean arterial blood pressure, as is the vascular resistance of the organism as a whole (257). A correlation between the increased values for cerebrovascular resistance and the degree of retinal vascular changes has been reported (195). This correlation suggests, just as does general clinical experience, that inspection of the retinal vessels may give some idea of the state of the cerebral vascular bed. A positive correlation between cerebral blood flow and cerebral oxygen consumption has been reported in a series of unilateral studies of patients with essential hypertension (122). Excluding the influence of random technical errors in the nitrous oxide method (which alone might explain the phenomenon) this correlation signifies that the cerebral arteriovenous oxygen difference is not inversely proportional to the cerebral blood flow. The results obtained in a series of bilateral studies are of some help in evaluating the significance of this finding (234). Analyzing the 34 bilateral studies in a heterogeneous group of subjects without evidence of intracranial vascular shunts, it was found that the jugular vein with the highest cerebral blood flow tended also to have the largest arteriovenous oxygen difference (r = 0.36; 0.05 > P > 0.02); Thus the side with the highest cerebral blood flow value usually also had the highest value for cerebral oxygen uptake (r = 0.82; P < 0.001). Hence it follows that true side-to-side differences may explain the above mentioned findings in patients with essential hypertension (122). It may well be, however, that some degree of real variation in cerebral oxygen uptake was present independent of side-to-side variations. If so, cerebral perfusion would presumably vary in parallel with the variations of the metabolic demand. But, owing to the above mentioned relationships, such a correlation cannot readily be disclosed.
* 原发性高血压。* 在没有脑部并发症的原发性高血压患者中,脑血流量和氧摄取量是正常的(122,166,172)。这意味着脑血管阻力的增加与平均动脉血压的增加成正比,整个机体的血管阻力也是如此(257)。已有报道说,脑血管阻力值的增加与视网膜血管变化的程度之间存在相关性(195)。这种相关性表明,正如一般的临床经验一样,对视网膜血管的检查可以对脑血管床的状况有一些了解。在一系列对原发性高血压患者的单侧研究中,已经报道了脑血流量和脑耗氧量之间的正相关关系(122)。排除氧化亚氮方法中随机技术错误的影响(仅此一项就可以解释这一现象),这种相关性标志着脑动静脉氧差与脑血流不成反比。在一系列双侧研究中获得的结果对评价这一发现的意义有一定帮助(234)。分析在一组没有颅内血管分流证据的异质受试者中进行的 34 项双侧研究,发现脑血流最高的颈静脉往往也有最大的动静脉氧差(r=0.36;0.05>P>0.02);因此脑血流值最高的一侧通常也有最高的脑氧摄取值(r=0.82;P<0.001)。因此,真正的侧向差异可能解释了上述原发性高血压患者的发现(122)。然而,很可能在某种程度上,脑氧摄取量的真正变化是独立于侧向变化的。如果是这样,脑灌注大概会与代谢需求的变化平行变化。但是,由于上述关系,这种关联性不容易被发现。
Essential hypertension complicated by severe headache is apparently not associated with abnormal values for cerebral perfusion and oxygen uptake (233). Acute hypertensive encephalopathy has already been discussed, and it was mentioned that the cerebral oxygen uptake was reduced in this condition (206, 228). Patients with chronic brain syndrome and arterial hypertension have reduced values for cerebral oxygen uptake and cerebral blood flow and very high values for the cerebral vascular resistance (309).
伴有严重头痛的基本高血压显然与脑灌注和摄氧量的异常值无关(233)。急性高血压脑病已经讨论过了,并提到在这种情况下脑氧摄取量减少(206,228)。慢性脑综合征和动脉高血压患者的脑氧摄取量和脑血流量的数值降低,而脑血管阻力的数值非常高(309)。
The regulation of the cerebral blood flow in essential hypertension has been studied intensively. Moderate tilting head-up has been found to cause a mild reduction in cerebral perfusion both before and after sympathectomy (126). Carbon dioxide inhalation has been found to increase cerebral blood flow as much as in normotensive subjects (241). Other investigators have reported a decreased carbon dioxide reactivity (66, 127, 131), but available data on the induced changes of the arterial pCO2 (127, 131) suggest that the cerebral circulation did actually react normally. The vasodilating effect of acutely induced hypotension has been established in numerous studies, demonstrating that this effect is independent of the agent used in producing the hypotension (23, 24, 29, 31, 49, 54, 55, 57, 80, 81, 125, 128, 130, 168, 179, 213, 223, 224, 228, 232, 332). Thus in hypertensive patients, just as in normotensive subjects, the fall in blood pressure induced by spinal anesthesia (168) was found to cause a similar reduction of cerebrovascular resistance, as, e.g., hexamethonium bromide (55, 57, 80, 213, 223, 224, 332). The effects of sympathectomy and/or subtotal adrenalectomy have also been studied. Both forms of treatment are followed by a significant reduction of the cerebrovascular resistance, so that cerebral perfusion is maintained at the normal level in spite of a moderate drop in mean arterial blood pressure (129, 305).
原发性高血压的脑血流调节已被深入研究。已发现在交感神经切除术之前和之后,适度的仰头会导致大脑灌注的轻度减少(126)。已发现吸入二氧化碳可使脑血流增加,与正常血压的受试者一样多(241)。其他研究者报告了二氧化碳反应性的降低(66,127,131),但是关于动脉 pCO2 的诱导性变化的现有数据(127,131)表明,脑循环实际上确实反应正常。许多研究已经证实了急性诱导性低血压的血管扩张效应,证明这种效应与产生低血压的药剂无关(23, 24, 29, 31, 49, 54, 55, 57, 80, 81, 125, 128, 130, 168, 179, 213, 223, 224, 228, 232, 332)。因此,在高血压患者中,就像在正常血压受试者中一样,发现脊柱麻醉(168)引起的血压下降会导致类似的脑血管阻力下降,例如,六甲溴铵(55,57,80,213,223,224,332)。交感神经切除术和 / 或肾上腺次全切除术的效果也已被研究。这两种形式的治疗都会使脑血管阻力明显降低,因此尽管平均动脉血压适度下降,但脑灌注仍保持在正常水平(129,305)。
It has been clearly shown that patients with essential hypertension are abnormal insofar as they cannot tolerate a blood pressure reduction to as low pressure levels as can normotensive subjects (cf. 81). This indicates that the cerebral blood vessels are unable to relax normally, presumably because of increased rigidity (81). When seen in relation to their habitual blood pressure, however, the tolerance of the hypertensive subjects was the same as in the normotensive group. In both groups a reduction of about 50 per cent in the initial blood pressure was required in order for clinical symptoms of cerebral circulatory failure to develop. Concomitantly, a critical reduction of the cerebral blood flow to about 60 per cent of the initial value was also found in both groups.
已经清楚地表明,原发性高血压患者是不正常的,因为他们不能像正常血压患者那样忍受血压降低到低压水平(参见 81)。这表明脑血管不能正常放松,可能是由于僵硬程度增加(81)。然而,当看到与他们的习惯血压有关时,高血压受试者的耐受性与正常血压组相同。在这两组中,最初的血压需要降低约 50%,才能出现脑循环衰竭的临床症状。同时,两组都发现脑血流临界值减少到初始值的 60% 左右。
The effect of more prolonged hypotensive therapy has also been studied. After several weeks of intensive treatment of elderly hypertensive patients, hypoxic cerebral symptoms developed at the same level of blood pressure reduction as before the treatment (180).
也有人研究过更长时间的降压治疗的效果。老年高血压患者经过几周的强化治疗后,在与治疗前相同的血压降低水平下出现了缺氧性脑症状(180)。
The cerebral circulation in essential hypertension seems to be adapted so that the perfusion is regulated in a normal fashion at the increased level of pressure. The abnormal cerebrosvascular rigidity demonstrated by acutely induced hypotension is intriguing. It would be of considerable interest to know whether a very prolonged efficient antihypertensive treatment would normalize the tolerance to hypotension.
原发性高血压的脑循环似乎是适应的,因此在压力增加的情况下,灌注的调节方式是正常的。急性诱发的低血压所表现出的脑血管异常僵硬是令人好奇的。我们很有兴趣知道,长期有效的降压治疗是否会使对低血压的耐受性恢复正常。
The above mentioned studies of the cerebral circulation in essential hypertension have not shed any light on the etiology of this disorder. The fact that cerebral circulation is regulated normally at the increased level of pressure does not necessarily indicate the action of a general humoral vasoconstrictor on the cerebral vessels. For, as indicated in the section on the regulation of the cerebral blood flow, this kind of adaptation would presumably be found in hypertension irrespective of the etiology.
上述对原发性高血压的脑循环的研究并没有对这种疾病的病因作出任何说明。在压力增加的情况下,脑循环的调节是正常的,但这并不一定表明一般体液性血管收缩剂对脑血管的作用。因为,正如关于脑血流调节的部分所指出的,这种适应性可能会在高血压中发现,而不论其病因如何。
Hypertensive toxemia of pregnancy. In normal pregnancy and in hypertensive toxemia without eclampsia, the cerebral blood flow and oxygen uptake are normal (203-212, 337). In patients with eclampsia, the cerebral oxygen uptake is reduced, while the cerebral blood flow remains normal (46, 206; see also the discussion of acute hypertensive encephalopathy). The effect of morphine, barbiturates, dihydrogenated ergot alkaloids and papaverine on the cerebral circulation and metabolism seems to be the same in patients with toxemia as in normal man (205, 207-212, 337; cf. the section on the action of drugs).
* 在正常怀孕和没有子痫的高血压毒血症中,脑血流和氧摄取量是正常的(203-212,337)。在子痫患者中,脑氧摄取量减少,而脑血流保持正常(46,206;也见对急性高血压脑病的讨论)。吗啡、巴比妥类药物、双氢化麦角生物碱和罂粟碱对脑循环和代谢的影响在毒血症患者中似乎与正常人相同(205, 207-212, 337;参见药物作用部分)。
Intense relative hypotension—an approximately 50 per cent reduction of the mean arterial blood pressure—induced by veratrum alkaloids or Apresoline (Z-hydrazinoptalazine) was found to cause no decrease of cerebral blood flow, and no hypoxic cerebral symptoms developed (206). This observation is of interest in relation to the above discussion of the tone of the cerebral vessels in essential hypertension. It seems to indicate that the ability of the cerebral vessels to relax normally is maintained in the relatively short-lived hypertensive state of hypertensive toxemia of pregnancy.
激烈的相对性低血压 -- 由藜芦生物碱或阿普唑啉(Z-hydrazinoptalazine)引起的平均动脉血压降低约 50%,发现没有引起脑血流减少,也没有出现缺氧性脑症状(206)。这一观察结果与上述关于基本高血压中脑血管张力的讨论有关。它似乎表明,在妊娠高血压毒血症的相对短暂的高血压状态下,脑血管的正常松弛能力得以维持。
Thyroid diseases. Several clinical studies of the cerebral circulation and oxygen metabolism have been reported (274, 285, 297, 324). Scheinberg and his coworkers reported normal values of cerebral oxygen uptake and cerebral blood flow in hyperthyroidism, and decreased values in hypothyroidism (274, 285). Sokoloff and associates found an increase in cerebral perfusion, but no increase in cerebral oxygen uptake in hyperthyroidism (324). In the most extensive study so far reported, Sensenbach et al. found that the cerebral oxygen uptake was not measurably changed in thyroid diseases, whereas the cerebral perfusion was increased in hyperthyroidism and decreased in hypothyroidism (297).
* 甲状腺疾病。* 对脑循环和氧代谢的一些临床研究已有报道(274,285,297,324)。Scheinberg 和他的同事报告说,在甲状腺功能亢进症中,脑氧摄取量和脑血流量的数值正常,而在甲状腺功能减退症中,数值下降(274,285)。Sokoloff 和他的同事发现甲状腺功能亢进症患者的脑灌注量增加,但脑氧摄取量没有增加(324)。在迄今为止报道的最广泛的研究中,Sensenbach 等人发现,在甲状腺疾病中,脑氧摄取量没有明显的变化,而在甲状腺功能亢进症中,脑灌注量增加,在甲状腺功能减退症中则减少(297)。
The apparent lack of influence of the thyroid hormone on cerebral oxygen uptake in adults is of considerable theoretical interest. Mental symptoms may be prominent in thyroid diseases, but seemingly these mental symptoms are not associated with changes of the total cerebral energy requirements as measured by the cerebral oxygen uptake. Animal studies have demonstrated that the thyroid hormone causes the cerebral oxygen uptake to rise more rapidly from the postnatal level to the adult level, whereas, in the mature animal, hyperthyroidism did not influence the cerebral oxygen uptake (67). That also the immature human brain is quite sensitive to lack of thyroid hormone is borne out by the marked mental retardation of cretins. So far no quantitative studies of the cerebral circulation and metabolism in this disorder have been published, but judging from the semiquantitative studies of Himwich and co-workers, the cerebral oxygen uptake is subnormal in cretinism (143).
甲状腺激素对成年人的脑氧摄取量明显缺乏影响,这在理论上有很大的意义。在甲状腺疾病中,精神症状可能很突出,但似乎这些精神症状与由脑摄氧量测量的大脑总能量需求变化无关。动物研究表明,甲状腺激素会使脑氧摄取量从出生后的水平更快地上升到成年水平,而在成熟动物中,甲状腺功能亢进并不影响脑氧摄取量(67)。未成熟的人脑对甲状腺激素的缺乏也相当敏感,这一点从雪貂的明显智力迟钝中得到了证实。到目前为止,还没有关于这种疾病的脑循环和新陈代谢的定量研究发表,但从 Himwich 和同事的半定量研究来看,克汀病的脑氧摄取量是不正常的(143)。
The observed changes of cerebral perfusion in thyroid disease in adults is puzzling. No adequate explanation for these changes have been demonstrated, as the chemical composition of the arterial blood and the arterial blood pressure was found to remain normal in the above mentioned studies (274, 285, 297, 324).
在成人甲状腺疾病中观察到的脑灌注变化是令人困惑的。对这些变化没有充分的解释,因为在上述研究中发现动脉血的化学成分和动脉血压保持正常(274, 285, 297, 324)。
Cardiac and pulmonary diseases. In compensated heart disease normal values for cerebral perfusion and oxygen uptake have been reported (39, 40, 226, 273). The reduced values found in patients with compensated aortic stenosis are presumably due to concomitant cerebral disease (40, 183). Severe cardiac decompensation without mental symptoms does not cause significant change of cerebral blood flow and oxygen uptake relative to the values obtained in comparable control groups (39, 40, 226, 227, 240, 273).
* 在代偿性心脏病中,脑灌注和摄氧量的正常值已被报告(39、40、226、273)。在代偿性主动脉瓣狭窄患者中发现的数值降低,可能是由于同时存在脑部疾病(40,183)。没有精神症状的严重心脏失代偿不会导致脑血流和摄氧量相对于可比对照组的数值有明显变化(39, 40, 226, 227, 240, 273)。
In cardiac failure causing marked mental symptoms, such as confusion, a decrease of cerebral blood flow has been found, whereas the cerebral oxygen uptake was not significantly decreased (60). In these patients the cerebral blood flow returned to the normal level following adequate therapy, relieving the cardiac failure and restoring normal mental function. Patients with cardiac failure and Cheyne-Stokes respiration have been found to have values for cerebral perfusion and oxygen uptake similar to those of cardiac patients with normal respiratory rhythm (227). Theophylline was found temporarily to abolish the Cheyne-Stokes respiration in these patients and to cause a reduction of cerebral blood flow, just as in normal man (227).
在心力衰竭引起明显的精神症状,如精神错乱,已经发现脑血流减少,而脑氧摄取量没有明显减少(60)。在这些病人中,经过适当的治疗后,脑血流量恢复到正常水平,缓解了心力衰竭,恢复了正常的精神功能。已发现心力衰竭和 Cheyne-Stokes 呼吸的病人的脑灌注和摄氧量的数值与呼吸节律正常的心脏病人相似(227)。发现茶碱能暂时取消这些病人的 Cheyne-Stokes 呼吸,并导致脑血流减少,就像正常人一样(227)。
Only few studies have been reported on congenital heart disease demonstrating adequate cerebral perfusion (39, 40, 123). High values for cerebral oxygen uptake and cerebral bood flow have been found in coarctation of the aorta (123). As only two cases were reported, it is not easy to evaluate the significance of these findings.
只有少数关于先天性心脏病的研究报告显示脑灌注充足(39,40,123)。在主动脉夹层中发现脑氧摄取量和脑血流的高值(123)。由于只有两例报告,因此不容易评估这些发现的意义。
Pulmonary insufficiency of a moderate degree does not affect the cerebral blood flow or oxygen uptake (280). In severe pulmonary failure with marked cor pulmonale and pronounced arterial hypercapnia and hypoxia an increase of cerebral blood flow was found, whereas the cerebral oxygen uptake remained normal (250). If normal subjects were acutely exposed to such changes of the blood gases as found in these two studies of chronic pulmonary diseases, then the cerebral blood flow would be expected to increase much more. This means that the cerebral circulation in patients with chronic arterial hypercapnia and hypoxia is in part adapted to the abnormal chemical milieu. The cerebral vessels of such patients are, however, still reactive to hypercapnia. Oxygen inhalation administered to the group of patients with the severest degree of pulmonary insufficiency resulted in normalization of the arterial oxygen saturation, a decrease in ventilation and a further increase in arterial pCO2 and in cerebral blood flow (250). The cerebral depression which may be seen when giving oxygen to such patients is caused by the extreme hypercapnia due to a critical reduction of pulmonary ventilation.
中度的肺功能不全并不影响脑血流或摄氧量(280)。在有明显的肺心病和明显的动脉高碳酸血症和低氧的严重肺衰竭中,发现脑血流量增加,而脑氧摄取量保持正常(250)。如果正常人被急性暴露在这两项慢性肺部疾病研究中发现的血气变化中,那么脑血流将被预期增加得更多。这意味着慢性动脉性高碳酸血症和低氧血症患者的脑循环部分地适应了异常的化学环境。然而,这些病人的脑血管对高碳酸血症仍有反应。对肺功能不全程度最严重的一组病人进行氧气吸入,使动脉血氧饱和度恢复正常,通气量减少,动脉 pCO2 和脑血流量进一步增加(250)。给这类病人输氧时可能出现的脑抑制是由于肺通气量严重减少而导致的极度高碳酸血症。
Anemia and polycythemia. In anemia and polycythemia the cerebral blood flow is increased and decreased respectively. The mechanism of these changes of perfusion have been discussed in the section on the regulation of the cerebral blood flow. The cerebral oxygen uptake has been found to be reduced in anemia, but normal in polycythemia (137, 238, 261, 275, 292). The low value for cerebral oxygen uptake in anemia deserves further comment. It has been reported both in pernicious anemia (275) and in sickle cell anemia (137), as well as in other types of anemia. Of special interest is the finding of subnormal values for the cerebral oxygen uptake in a group of 18 young anemic patients, the majority of whom had simple iron deficiency anemia (137). No mental symptoms were reported, nor were they likely to have been present, as the degree of anemia was not extreme.
* 贫血和多血症。在贫血和多血症中,脑血流量分别增加和减少。这些灌注变化的机制已在脑血流调节一节中讨论过。已发现贫血时脑氧摄取量减少,而多血症时则正常(137, 238, 261, 275, 292)。贫血时脑氧摄取量的低值值得进一步评论。在恶性贫血(275)和镰状细胞贫血(137)以及其他类型的贫血中,都有这种报道。特别值得注意的是,在一组 18 名年轻的贫血患者中,发现脑氧摄取量低于正常值,其中大多数是单纯的缺铁性贫血(137)。由于贫血程度不是很严重,所以没有报告精神症状,也不可能有精神症状。
Probably the low values for cerebral oxygen uptake found in uncomplicated anemia are due to technical errors. The nitrous oxide method was used in all these studies without correction for the lower solubility of nitrous oxide in anemic blood or for the fact that high perfusion values would cause the heterogeneity of the cerebral blood flow to influence the perfusion values less than in normal man. These two factors have both been discussed in the section on the inert gas method. It can be estimated that an underestimation of cerebral perfusion and oxygen uptake of about 10-20 per cent will result, if no correction for the influence of these two factors are employed in patients with marked anemia. This explains why the observed value of cerebral oxygen uptake increases when the anemia is corrected (275), and also why oxygen inhalation in anemia, which reduces the cerebral perfusion, causes a slight increase in cerebral oxygen uptake (137).
在无并发症的贫血中发现的脑氧摄取量的低值可能是由于技术错误造成的。在所有这些研究中都使用了一氧化二氮法,而没有对一氧化二氮在贫血中的溶解度较低进行校正,也没有对高灌注值会导致脑血流的异质性对灌注值的影响小于正常人的事实进行校正。这两个因素都已在惰性气体法一节中讨论过。可以估计,如果不对这两个因素的影响进行校正,在有明显贫血的病人中,将导致对脑灌注和摄氧量的低估,大约为 10-20%。这就解释了为什么纠正了贫血后,脑摄氧量的观察值会增加(275),也解释了为什么贫血时吸入氧气,减少了脑灌注,会导致脑摄氧量的轻微增加(137)。
Presumably some of the aged patients with pernicious anemia studied had some degree of chronic cerebral disease, as the values remained moderately subnormal even after correction of the anemia (275). It is not possible to come to any conclusion regarding the cause of the chronic brain disease in these patients.
据推测,所研究的一些老年恶性贫血患者有某种程度的慢性脑病,因为即使在纠正了贫血后,其数值仍处于中等偏下水平(275)。对于这些病人的慢性脑部疾病的原因,我们不可能得出任何结论。
# 药物对脑血流和摄氧量的作用
Action of Drugs on Cerebral Blood Flow and Oxygen Uptake
# 一般麻醉剂和其大脑抑制剂
General Anesthetics and Other Cerebral Depressants
The effect of the various drugs which can cause a depression of the level of consciousness to the extent of semicoma or coma is well exemplified by the effect of barbiturates. Regardless of the specific drug used—amytal, phenobarbital, thiopental, etc.,—and regardless of the doses used, the barbiturates all cause a reduction of the cerebral oxygen uptake which correlates with the degree of cerebral depression. Light sedation reduces the cerebral oxygen uptake only a few percentages, a reduction which was not found to be statistically significant (176, 210); marked sedation, causing loss of consciousness when the subject is not exposed to painful stimuli, results in a significant (about 25 %) reduction of cerebral oxygen uptake (210). Surgical anesthesia reduces the cerebral oxygen uptake by about 40-50 per cent (19, 145, 289, 343).
各种药物的作用可以导致意识水平的抑制,达到半昏迷或昏迷的程度,巴比妥酸盐的作用就是很好的例证。无论使用何种具体药物 -- 阿米妥、苯巴比妥、硫喷妥等,也无论使用何种剂量,巴比妥类药物都会导致脑氧摄取量的减少,这与脑抑制的程度有关。轻度镇静只减少了几个百分点的脑氧摄取量,这种减少在统计学上没有意义(176,210);明显的镇静,在受试者没有受到痛苦刺激时造成意识丧失,导致脑氧摄取量明显减少(约 25%)(210)。手术麻醉会使脑氧摄取量减少约 40-50%(19, 145, 289, 343)。
In all these studies, cerebral blood flow was found to be relatively less reduced than the cerebral oxygen uptake. This lack of proportionate reduction in perfusion is probably due to a barbiturate-induced hypoventilation. This is evidenced by a rise in the arterial pCO2 found in all the studies where this value was reported. This hypoventilation was especially pronounced in the study by Wechsler and collaborators, in which the cerebral blood flow values actually rose slightly above the control values. In animal experiments where artificial ventilation was maintained, pentothal anesthesia was found to cause a relatively more pronounced reduction of cerebral blood flow than of cerebral oxygen uptake (294).
在所有这些研究中,发现脑血流量的减少相对少于脑氧摄取量。这种缺乏比例的灌注量的减少可能是由于巴比妥酸盐引起的通气不足。在所有报告该值的研究中,动脉 pCO2 的上升就证明了这一点。这种通气不足在 Wechsler 和合作者的研究中特别明显,其中脑血流值实际上略高于对照值。在保持人工通气的动物实验中,发现戊四醇麻醉引起的脑血流减少比脑氧摄取量减少相对更明显(294)。
Severe acute barbiturate poisoning is rarely followed by permanent brain damage. An increased cerebral blood flow due to arterial hypercapnia and hypoxia and a low cerebral oxygen demand presumably protect the brain against noxious influences of the severe hypotension and hypoxia found in such patients.
严重的急性巴比妥酸盐中毒后很少出现永久性的脑损伤。由于动脉高碳酸血症和低氧血症导致的脑血流量增加以及低的脑氧需求可能会保护大脑免受在这类病人中发现的严重低血压和低氧血症的有害影响。
No reports have been published concerning the influence of volatile anesthetics on the perfusion and oxygen uptake in the human brain. Animal studies reviewed by Sokoloff strongly suggest that the drugs have the same effect on the cerebral oxygen uptake as the barbiturates. Changes of cerebral perfusion, however, depend also upon the influence on the pulmonary gas exchange of the particular drug (318). General anesthesia induced by the steroid 21-hydroxypregnane-3,20-dione sodium succinate has been found to cause about a 50 per cent reduction of the cerebral blood flow and oxygen uptake in man (111, 115).
目前还没有关于挥发性麻醉剂对人脑灌注和氧摄取的影响的报告发表。由 Sokoloff 回顾的动物研究强烈表明,这些药物对脑氧摄取的影响与巴比妥类药物相同。然而,脑灌注的变化也取决于特定药物对肺部气体交换的影响(318)。由类固醇 21 - 羟基孕甾 - 3,20 - 二酮琥珀酸钠引起的全身麻醉已被发现导致人的脑血流和氧摄取量减少约 50%(111,115)。
The cerebral oxygen uptake is reduced in severe methyl or ethyl alcohol intoxication (13, 14, 15) and also in the Antabuse3 ethyl alcohol reaction (146). A moderate dose of ethyl alcohol producing a blood concentration of o. 1 per cent has no significant effect on cerebral perfusion or oxygen uptake (13, 14, 62), even when given in combination with 100 mg chlorpromazine (62).
在严重的甲基或乙基酒精中毒中,脑氧摄取量减少(13,14,15),在安泰宝 [3](#bookmark6)乙基酒精反应中也是如此(146)。中等剂量的乙醇产生的血药浓度为 o.1%,对脑灌注或氧摄取没有明显影响(13,14,62),即使与 100 毫克氯丙嗪合用(62)。
Small analgesic doses of Methadon and morphine do not change the cerebral blood flow or oxygen uptake under normal conditions (1, 209). The effect of such doses of morphine in hemorrhagic shock (331) has already been mentioned. Heavy doses of Demerol (pethidine) have been used in combination with chlorpromazine, phenergan and cooling in the so called artificial hibernation. In these conditions the cerebral oxygen uptake and blood flow are reduced (22, 77, 119, 316). Morphine in doses (60 mg) causing distinct depression of mental function and of respiration also decreases the CMRO2, while the CBF. is unaffected (229b). The hypoventilation caused an average rise in arterial carbon dioxide tension from 43 to 52 mm Hg. This hypercapnia may well be of importance for maintaining the cerebral blood flow at a high level. The effect of 25 mg n-allylmorphine on morphine intoxication was studied in the same subjects, and a rapid but only partial reversal of the metabolic and mental depression was observed.
小剂量镇痛剂美沙酮和吗啡在正常情况下不改变脑血流或氧摄取量(1,209)。这种剂量的吗啡对失血性休克(331)的影响已经提到。大剂量的杜冷丁(哌替啶)已与氯丙嗪、酚丁胺和冷却剂一起用于所谓的人工冬眠。在这些条件下,脑氧摄取量和血流量减少(22,77,119,316)。吗啡的剂量(60 毫克)导致精神功能和呼吸的明显抑制,也降低了 CMRO2,而 CBF 不受影响(229b)。通气不足导致动脉二氧化碳张力从 43 毫米汞柱平均上升到 52 毫米汞柱。这种高碳酸血症很可能对维持高水平的脑血流有重要意义。在同一受试者中研究了 25 毫克正烯丙基吗啡对吗啡中毒的影响,观察到代谢和精神抑制的迅速但只是部分逆转。
A hypothesis of the action of anesthetic drugs has been formulated on the basis of the above mentioned in vivo experiments and certain in vitro observations. Barbiturate-induced depression of oxygen uptake of isolated nervous tissues in vitro (258) requires much higher substrate concentrations than the blood concentrations causing a proportionate reduction of cerebral oxygen uptake in vivo (19, 145, 210, 289, 343; see also 187). Also, a substrate concentration of 6.0% ethyl alcohol is required in order to reduce the oxygen uptake of isolated cerebral tissues to about two-thirds of the control value (144), while a similar reduction in vivo results when the blood alcohol level is only 0.3% (13). These observations support the hypothesis that in vivo the anesthetic drugs in low concentrations depress the function of the synapses, thus reducing the number of nervous impulses and hence the cerebral oxygen demand. In the in vitro state, where spontaneous neuronal impulses and synaptic transmissions are absent, much higher concentrations are required to reduce the low level of resting oxygen uptake.
在上述体内实验和某些体外观察的基础上,提出了麻醉药物作用的假说。巴比妥引起的离体神经组织摄氧量的抑制在体外(258)需要比血液浓度高得多的底物浓度,导致大脑摄氧量的比例减少在体内(19,145,210,289,343;也见 187)。另外,需要 6.0% 的乙醇底物浓度才能使离体脑组织的摄氧量减少到控制值的三分之二左右(144),而当血液中的酒精含量仅为 0.3% 时,体内会出现类似的减少(13)。这些观察结果支持这样的假设:在体内低浓度的麻醉药物会抑制突触的功能,从而减少神经冲动的数量,从而减少脑部的需氧量。在体外 * 的状态下,由于没有自发的神经冲动和突触传递,需要更高的浓度来减少低水平的静止氧摄取。
# 直接作用于大脑的其他药物
Other Drugs Acting Directly on the Brain
The effect of convulsant drugs (e.g. strychnine, picrotoxin, Metrazol, Nikethamide) on the cerebral blood flow and oxygen uptake has not been studied in man (see 318). Probably the most accurate animal studies were made by Schmidt and his co-workers, using the bubble flow-meter technique, in lightly anesthetized monkeys (59, 294). Cerebral oxygen uptake and blood flow were invariably increased during the actual convulsions, while low values were found in the post-convulsive semicomatose state. In the absence of convulsions, even using large doses of convulsant drugs, no change of cerebral oxygen uptake or blood flow was observed. This indicates that it is the seizure, and not the drugs as such, which causes the observed cerebral metabolic and circulatory effects.
惊厥药物(如马钱子、微毒、甲硝唑、尼卡胺)对脑血流和氧摄取的影响尚未在人身上进行研究(见 318)。最准确的动物研究可能是由 Schmidt 和他的同事使用气泡流量计技术,在轻度麻醉的猴子身上进行的(59,294)。在实际抽搐期间,脑氧摄取量和血流量无一例外地增加了,而在抽搐后的半昏迷状态下发现的数值很低。在没有抽搐的情况下,即使使用大剂量的抽搐药物,也没有观察到脑氧摄取量或血流量的变化。这表明是癫痫发作,而不是药物本身,导致观察到的脑代谢和循环系统的影响。
The various psychotropic drugs studied seem to have no effect on the cerebral oxygen uptake or the cerebral blood flow in man. The lack of effect of sedative doses of the Rauwolfia alkaloid reserpine (130, 179) and the phenathiazine derivate chlorpromazine (62, 229a) is perhaps not surprising in view of the similar lack of influence of sedative doses of barbiturates (176, 210). Of more interest is the lack of effect of 100-120 micrograms of ^-lysergic acid diethylamide (LSD-25) (322). In these studies of normal as well as schizophrenic subjects, characteristic mental disturbances were produced as well as a slight pressor effect. The absence of a measurable change in cerebral oxygen uptake in this form of toxic psychosis is noteworthy, as it corroborates the previously mentioned findings of a lack of correlation between psychotic behavior and cerebral oxygen uptake in schizophrenia and in psychoses in elderly patients.
研究的各种精神药物似乎对人的脑氧摄取或脑血流没有影响。鉴于巴比妥类药物(176,210)的镇静剂量也没有影响,劳沃夫生物碱(130,179)和吩噻嗪衍生物氯丙嗪(62,229a)的镇静剂量没有影响,也许并不令人惊讶。更令人感兴趣的是 100-120 微克的 ^- 麦角酸二乙胺(LSD-25)没有影响(322)。在这些对正常人和精神分裂症受试者的研究中,产生了特征性的精神障碍以及轻微的压迫作用。在这种形式的中毒性精神病中没有可测量的脑氧摄取量的变化是值得注意的,因为它证实了之前提到的精神分裂症和老年精神病患者的精神病行为和脑氧摄取量之间缺乏相关性的发现。
# 黄嘌呤化合物
Xanthine Compounds
The xanthine compounds have a well recognized stimulatory effect on the mental functions of the brain, and have also a stimulatory effect on the respiratory center (344). Theophylline (with ethylendiamine) and caffeine cause a distinct reduction of the cerebral blood flow in man without changing cerebral oxygen uptake (66, 227, 233, 300, 344).4 It is possible that the xanthine compounds per se cause the cerebral vasoconstriction, as the hyperventilation observed was seemingly inadequate to produce the observed reduction of cerebral blood flow to about 75 per cent of the control values. Theophylline also decreases cerebral blood flow in cardiac patients with Cheyne-Stokes respiration (227, 231) and in patients with hypertensive headaches (233). The therapeutic effect on the Cheyne-Stokes respiration is presumably due to a direct stimulation of the respiratory center, whereas in the case of patients with hypertensive headache the therapeutic effect of theophylline may be due to the decreased distention of the pain receptors adjoining the cerebral arteries.
黄嘌呤化合物对大脑的精神功能有公认的刺激作用,而且对呼吸中枢也有刺激作用(344)。茶碱(与乙二胺)和咖啡因导致人的脑血流明显减少,而不改变脑氧摄取量(66,227,233,300,344)。[4](#bookmark7)可能是黄嘌呤化合物本身导致脑血管收缩,因为观察到的过度通气似乎不足以产生观察到的脑血流减少到控制值的 75% 左右。茶碱也会使有 Cheyne-Stokes 呼吸的心脏病患者(227,231)和高血压头痛患者(233)的脑血流量减少。对 Cheyne-Stokes 呼吸的治疗作用可能是由于对呼吸中枢的直接刺激,而在高血压头痛患者中,茶碱的治疗作用可能是由于与脑动脉相邻的疼痛感受器的膨胀减少。
# 降压药物和其他血管扩张药物
Anti-Hypertensive Drugs and Other Vasodilator Drugs
The various vasodilator drugs have no direct influence on the cerebral oxygen uptake. The influence on the cerebral circulation is in most cases nonspecific, i.e., the response depends only on the degree of hypotension achieved and not on the drug or dose employed (see e.g. 230). This suggests that most vasodilator drugs have no significant direct effect on the cerebral vessels,and that the cerebrovascular relaxation observed is due to the effect of the hypotension. This conclusion is supported by observations demonstrating a similar cerebrovascular relaxation during acute hypotension induced by spinal anesthesia (168, 184, 185), a procedure which can hardly be expected to have any direct influence on the cerebrovascular tone.
各种血管扩张药物对脑氧摄取没有直接影响。对脑循环的影响在大多数情况下是非特异性的,即反应只取决于所达到的低血压程度,而不取决于所使用的药物或剂量(见例如 230)。这表明大多数血管扩张药物对脑血管没有明显的直接作用,观察到的脑血管松弛是由于低血压的影响。这一结论得到了观察结果的支持,这些观察结果表明,在脊髓麻醉引起的急性低血压期间,也有类似的脑血管松弛现象(168,184,185),这种手术很难对脑血管张力产生任何直接影响。
::::
7 Parephylline (diethyl-aminoethyl-theophylline-HCl) has been studied in a small series of cases, and was found to cause no change of cerebral perfusion, but to increase the cerebral oxygen uptake 25% (231). These divergent observations are surprising, as the drug presumably has the same effect as theophylline. Additional observations on parephylline seem to be indicated.
7 帕雷菲林(二乙胺基乙基茶碱 - 盐酸)曾在一个小系列的病例中被研究,发现没有引起脑灌注的变化,但增加了 25% 的脑氧摄取量(231)。这些不同的观察结果令人惊讶,因为该药物可能具有与茶碱相同的效果。对帕瑞林的其他观察似乎是有意义的。
The regulation of cerebral circulation in moderate and severe hypotension induced by drugs or by other means has been discussed previously. The observation that patients with essential hypertension have a reduced tolerance to an acute reduction of the blood pressure has also been mentioned. This section gives only the references to the many quantitative studies of the circulation of the human brain during hypotension induced by the various antihypertensive drugs of seemingly unspecific action. Other vasodilator drugs, a few of which appear to exert an independent and direct dilative action on the cerebral vessels, will be discussed subsequently.
前面已经讨论过由药物或其他手段诱发的中度和重度低血压的脑循环调节问题。还提到了原发性高血压患者对血压急性下降的耐受性降低的观察。本节仅提及在各种看似无特异性作用的抗高血压药物诱导的低血压期间,对人脑循环的许多定量研究。其他血管扩张药物,其中一些似乎对脑血管有独立和直接的扩张作用,将在随后讨论。
Some ganglionic blocking agents have been studied in normotensive as well as in hypertensive subjects: Tetraethyl ammonium (31), hexamethonium (55, 57, 80, 81, 148, 213, 223, 224, 229, 230, 332), Pendiomide (24, 29, 229, 230), and trimethaphan (Arfonad) (213, 229, 230). Of the various adrenergic blocking agents, only Dibenzyline (phenoxybenzamine) (232) and dihydrogenated ergot alkaloids (1, 124, 125) have been studied. Miscellaneous other antihypertensive drugs studied include 1-hydralazine (Apresoline) (128, 206), veratrum alkaloids (54, 206, 228) and rauwolfia alkaloids (130, 179).
一些神经节阻断剂已在正常血压和高血压患者中进行了研究。四乙基铵(31)、六甲基铵(55、57、80、81、148、213、223、224、229、230、332)、奔地米(24、29、229、230)和三甲胺(Arfonad)(213、229、230)。在各种肾上腺素能阻断剂中,只有 Dibenzyline(苯氧苄胺)(232)和双氢化麦角生物碱(1,124,125)被研究。所研究的其他杂项降压药物包括 1 - 肼基拉嗪(Apresoline)(128,206)、藜芦生物碱(54,206,228)和乌头碱(130,179)。
The imidazoline compounds phentolamine (Regitine) and tolazoline (Priscoline) cause only a slight reduction of the blood pressure and have no decisive effect on the cerebral circulation (23, 49, 58, 278). Histamine, also an imidazoline compound, was found to cause distinct hypotension without significantly affecting cerebral blood flow in two groups of patients studied (8, 300). In one of these studies (300), however, moderate doses of histamine causing only a small decrease in blood pressure actually increased cerebral blood flow, possibly by direct vasodilatation.
咪唑啉化合物酚妥拉明(Regitine)和托拉佐林(Priscoline)只引起血压的轻微下降,对脑循环没有决定性的影响(23,49,58,278)。组胺,也是一种咪唑啉化合物,在两组病人的研究中发现会引起明显的低血压,而不明显影响脑血流(8,300)。然而,在其中一项研究中(300),中等剂量的组胺仅导致血压小幅下降,实际上增加了脑血流量,可能是通过直接的血管扩张。
The effect of nitrites has not been studied in man, but observations in experimental animals suggest a direct cerebral vasodilatory action in addition to the systemic effect (see 318). While nicotinic acid (270, 338) and procaine (282, 283) seem to have no effect on the cerebral circulation, the opium alkaloid papaverine has a distinct vasodilatory effect on the cerebral vessels, increasing the cerebral blood flow above the control level (149, 205, 207, 283, 300). Papaverine presumably acts directly on the cerebral vessels. This is not definitely proved, however, as in none of the studies referred to above has the possible influence of hypercapnia been excluded.
亚硝酸盐的作用尚未在人身上进行研究,但对实验动物的观察表明,除了全身性作用外,还有直接的脑血管扩张作用(见 318)。虽然烟酸(270,338)和普鲁卡因(282,283)似乎对脑循环没有影响,但鸦片生物碱罂粟碱对脑血管有明显的血管扩张作用,使脑血流量超过控制水平(149,205,207,283,300)。罂粟碱可能直接作用于大脑血管。然而,这一点并没有得到确切的证明,因为在上面提到的研究中,都没有排除高碳酸血症的可能影响。
# 激素和相关药物
Hormones and Related Drugs
Z-Nor-epinephrine in pressor doses does not change the cerebral oxygen uptake, but causes a moderate reduction of cerebral blood flow by reason of a slight drop in the arterial pCO2 (177, 230, 298) or by reason of an effect via the pressoreceptor reflexes affecting the resistance at the periphery and the cardiac output, exempting the cerebral vascular resistance. Z-Epinephrine administered intravenously in pressor doses has been found to cause a significant increase in cerebral perfusion and oxygen uptake (177). Other investigators found no effect when administering Z-epinephrine and USP epinephrine intramuscularly in oil, in doses causing a slight drop in mean arterial blood pressure (298). It is noteworthy that in both studies Z-epinephrine produced distinct symptoms of anxiety (177, 298).
Z - 去甲肾上腺素的加压剂量不改变脑氧摄取量,但由于动脉 pCO2 的轻微下降(177,230,298),或由于通过加压感受器反射影响周边阻力和心输出量而导致脑血流适度减少,免除了脑血管阻力。已发现静脉注射加压剂量的 Z - 肾上腺素会导致脑灌注和氧摄取量的明显增加(177)。其他研究者发现,在油中肌肉注射 Z - 肾上腺素和 USP 肾上腺素时,在引起平均动脉血压轻微下降的剂量中没有发现任何影响(298)。值得注意的是,在这两项研究中,Z - 肾上腺素产生了明显的焦虑症状(177,298)。
Some other sympathicomimetic amines have been studied. Amphetamine and Aramine (i-i-(w-hydroxyphenyl)-2-amino-1-propanol) were found to cause a rise in blood pressure without changing cerebral blood flow or oxygen uptake (1, 2, 230, 300). Mephentermine (N,a,a,-trimethylphenethylamine sulphate), however, was found to increase the cerebral oxygen uptake significantly without changing cerebral blood flow (73). Sympathicomimetic amines were able to normalize the blood pressure and the cerebral perfusion in patients in whom both values had been reduced by ganglionic blocking agents (230).
对其他一些拟交感神经胺类药物也进行了研究。安非他明和阿拉明(i-i-(w-hydroxyphenyl)-2-amino-1-propanol)被发现会导致血压上升而不改变脑血流或氧摄取量(1,2,230,300)。然而,美芬特明(N,a,a,- 三甲基苯乙胺硫酸盐)被发现在不改变脑血流的情况下明显增加脑氧摄取量(73)。拟交感胺类药物能够使血压和脑灌注恢复正常,而这两个数值都被神经节阻断剂降低了(230)。
Adrenocorticotropic Hormone (ACTH) and cortisone were found to increase the arterial blood pressure moderately, while the cerebral blood flow either remained unchanged or decreased slightly (7, 287, 299). The cerebral oxygen uptake remained unchanged in these studies. Vasopressin has been studied in only a few cases (323), showing no effect on cerebral blood flow despite a sustained pressor response.
肾上腺皮质激素(ACTH)和可的松被发现能适度增加动脉血压,而脑血流保持不变或略有下降(7, 287, 299)。在这些研究中,脑氧摄取量保持不变。血管加压素只在少数情况下被研究过(323),显示尽管有持续的加压反应,但对脑血流没有影响。
The injection of desoxycorticosterone does not affect the cerebral circulation or oxygen uptake (20). Gordan and associates reported preliminary studies of the effect of androgenic hormones (111, 112, 113) .The results are far from clear, and their interpretation must await further investigation permitting a statistical evaluation of the data. The effect of thyroxine has already been discussed in the section on thyroid diseases.
注射去氧皮质酮不影响脑循环和摄氧量(20)。Gordan 和他的同事报告了对雄性激素影响的初步研究(111,112,113)。结果还很不明确,对它们的解释必须等待进一步的调查,允许对数据进行统计评估。甲状腺素的影响已经在关于甲状腺疾病的章节中讨论过了。
# 其他药物
Miscellaneous Drugs
Heparin (336) does not affect cerebral circulation or oxygen uptake. Hypertonic solutions of sodium chloride (288) or glucose (311) cause an acute reduction in the hemoglobin concentration and a corresponding increase in cerebral perfusion.
肝素(336)不影响脑循环或摄氧量。氯化钠(288)或葡萄糖(311)的高渗溶液会引起血红蛋白浓度的急性降低,并相应增加脑灌注量。
# 药理学一般注意事项
General Pharmacological Considerations
In the preceding sections the action of drugs on cerebral blood flow and oxygen uptake in man has been briefly presented. The most important findings may be summarized:
在前面的章节中,已经简要介绍了药物对人的脑血流和氧摄取的作用。最重要的发现可以总结一下。
The cerebral oxygen uptake is relatively little influenced by drugs. Reduced values are found only in drug-induced semicoma and coma, while increased values only occur in drug-induced convulsions and during the intravenous infusion of large doses of /-epinephrine. Drug-induced changes in the cerebral oxygen uptake, the arterial blood pressure, the arterial pCO2, and the blood hemoglobin concentration cause the same changes of cerebral blood flow as discussed in the section on the regulation of the cerebral blood flow. An independent, direct effect of drugs on the cerebral circulation is rare, and in no case is marked. The direct vasodilator effect of the alkaloid papaverine is best established. Possibly histamine, nitrites and thyroxine have the same effect. Only the various xanthine compounds seem to cause a direct constriction of the cerebral vessels.
大脑摄氧量受药物的影响相对较小。只有在药物引起的半身不遂和昏迷时才会发现数值降低,而只有在药物引起的抽搐和静脉注射大剂量的 / 肾上腺素时才会出现数值升高。药物诱导的脑氧摄取量、动脉血压、动脉 pCO2 和血红蛋白浓度的变化引起的脑血流变化与在脑血流调节一节中讨论的相同。药物对脑循环的独立、直接影响是罕见的,而且在任何情况下都是明显的。生物碱帕帕弗林的直接血管扩张作用是最确定的。组胺、亚硝酸盐和甲状腺素也可能有同样的作用。只有各种黄嘌呤化合物似乎能引起脑血管的直接收缩。
# 结语
Concluding Remarks
Until about 1930 the cerebral circulation was generally believed to vary passively with changes in the perfusion pressure (18, 141). This concept was based mainly on the Monro-Kellie doctrine of a constant volume of the intracranial contents (151, 235), from which it was deduced that no significant changes in intracranial blood volume or vascular diameter were likely to occur. The possibility of redistribution of blood within the cerebral vascular bed or of an increase of blood volume at the expense of the transference of cerebrospinal fluid into the spinal channel was considered. No experimental data, however, were available to support such a contention.
直到 1930 年左右,人们普遍认为脑循环是随着灌注压的变化而被动变化的(18,141)。这一概念主要是基于 Monro-Kellie 关于颅内内容物体积恒定的学说(151,235),由此推断颅内血量或血管直径不可能发生明显变化。考虑到血液在脑血管床内的重新分布或以脑脊液转入脊髓通道为代价增加血容量的可能性。然而,没有实验数据支持这一论点。
Unequivocal evidence of active changes of vascular diameter of the cerebral vessels was first obtained by direct observation of the pial vessels through a cranial window, a technique developed by Forbes (89). As a result of these and other animal studies, a theory of a highly developed intrinsic control of cerebral circulation was developed. Two types of stimuli were found to be of importance for the physiological regulation of the myogenic tone of the vascular walls, namely, certain chemical agents, primarily carbon dioxide and oxygen (292), and the distending pressure (82). Neurogenic control of cerebrovascular resistance was studied extensively without it being possible to assign any definite physiological role to the cerebral perivascular nerves.
福布斯(Forbes)开发的一种技术,通过颅窗直接观察皮层血管,首次获得了脑血管直径主动变化的明确证据(89)。作为这些和其他动物研究的结果,一个高度发达的脑循环内在控制的理论被提出。人们发现有两类刺激对血管壁肌源性张力的生理调节很重要,即某些化学制剂,主要是二氧化碳和氧气(292),以及膨胀压力(82)。对脑血管阻力的神经源性控制进行了广泛的研究,但不可能给脑血管周围神经赋予任何明确的生理作用。
During the last decade quantitative studies in man have confirmed these results on all essential points. The cerebral perfusion in normal man varies only moderately, the most important regulating factor probably being the tissue carbon dioxide tensions and the direct reaction of the muscular cells of the cerebral arteries in response to variations of the distending blood pressure. The cerebral circulation has also been studied in many disease entities, and it appears in general that the cerebral perfusion is ample relative to the cerebral metabolism. Of particular interest is the finding of adequate over-all cerebral perfusion in so called cerebral arteriosclerosis. Only in severe hypotension and during marked hyperventilation has total cerebral perfusion been found to be critically lowered.
在过去的十年中,对人的定量研究证实了这些结果的所有基本点。正常人的脑灌注量变化不大,最重要的调节因素可能是组织的二氧化碳张力和脑动脉的肌肉细胞对膨胀血压变化的直接反应。对许多疾病实体的脑循环也进行了研究,一般来说,相对于脑代谢,脑灌注是充足的。特别有意思的是,在所谓的脑动脉硬化中发现了充分的整体脑灌注。只有在严重的低血压和明显的过度通气时,才发现总的脑灌注量严重下降。
These clinical studies have also given a wealth of information concerning the oxygen consumption of the human brain. This is of considerable interest, as studies in experimental animals had previously only permitted a rough estimate of this value under relatively abnormal experimental conditions. In normal man, not given pharmacological agents, the cerebral oxygen uptake is remarkably constant. With the possible exception of severe anxiety states, no significant changes of cerebral oxygen uptake have been reported in a variety of conditions studied. Thus, cerebral oxygen consumption is unchanged during sleep and during physical or intellectual effort, and also unaffected by relatively marked changes of the arterial blood pressure and gas tensions of the arterial blood. In all these conditions changes of cerebral blood flow are accompanied by inversely proportionate changes of the cerebral arteriovenous oxygen difference. This means that in such conditions it is possible to calculate changes in the cerebral perfusion from observations of variations of the cerebral arteriovenous oxygen difference. This method for evaluating changes of cerebral blood flow was proposed on a theoretical basis by Lennox and Gibbs as far back as 1932 (192). It may be useful, as it enables one to follow fairly rapid changes in cerebral blood flow (136, 247).
这些临床研究还提供了有关人脑耗氧量的大量信息。这是很有意义的,因为对实验动物的研究以前只允许在相对不正常的实验条件下对这个值进行粗略的估计。在正常人中,如果不使用药物,大脑的摄氧量是非常稳定的。除了严重的焦虑状态外,在各种研究条件下,脑氧摄取量没有明显变化。因此,在睡眠和体力或脑力劳动时,脑耗氧量是不变的,而且不受动脉血压和动脉血中气体张力相对明显变化的影响。在所有这些条件下,脑血流的变化都伴随着脑动脉血氧差的反比例变化。这意味着在这些条件下,可以通过观察脑动静脉氧差的变化来计算脑灌注的变化。这种评估脑血流变化的方法早在 1932 年就由 Lennox 和 Gibbs 在理论基础上提出(192)。它可能是有用的,因为它使人们能够跟踪脑血流的相当快速的变化(136,247)。
It has also been established that the cerebral oxygen uptake is subnormal only in acute and chronic cerebral disorders characterized by distinct signs of mental hypofunction, depression of consciousness in acute disorders, and loss of intellectual faculties in chronic disorders. Thus, correlation between mental function and the over-all energy expenditure of the brain in certain conditions has been established.
也已经确定,只有在急性和慢性脑部疾病中,脑氧摄取量才是不正常的,其特点是精神功能低下的明显迹象,急性疾病中的意识压抑,慢性疾病中的智力丧失。因此,在某些情况下,精神功能和大脑的总体能量消耗之间的相关性已经建立。
These major findings and the wealth of additional observations have very substantially increased our understanding of this important area of human physiology. Undoubtedly our knowledge is still incomplete at various points. However, a solid foundation for relevant physiological thinking and for future studies has been established.
这些主要的发现和大量的额外观察,大大增加了我们对人类生理学这一重要领域的了解。毋庸置疑,我们的知识在各方面仍然是不完整的。然而,我们已经为相关的生理学思考和未来的研究奠定了坚实的基础。
The author acknowledges gratefully the many helpful criticisms and suggestions made by Drs. Seymour Kety and Louis Sokoloff of the National Institute of Mental Health, and by Dr. Lawrence S. Lilienfield of the Cardiovascular Research Laboratory of Georgetown University Medical School. He also wishes to thank Dr. Sokoloff for making available to him unpublished data and his review on the pharmacology of the cerebral circulation.
作者感谢国家精神卫生研究所的西摩 - 凯蒂和路易斯 - 索科洛夫博士以及乔治敦大学医学院心血管研究实验室的劳伦斯 - S - 利连菲尔德博士提出的许多有益的批评和建议。他还要感谢索科洛夫博士向他提供了未发表的数据和他对脑循环药理学的评论。