
 细胞因子吸要废了吗?
细胞因子吸要废了吗?
# 细胞因子吸附要废了吗?
# Is This the Beginning of the End of Cytokine Adsorption?
# Jan T. Kielstein,Alexander Zarbock
# DOI:10.1097/CCM.0000000000005509
关键词:COVID-19;细胞因子吸附;器官衰竭;血管麻痹性休克
KEY WORDS: COVID-19; cytokine adsorber; organ failure; vasoplegic shock
温斯顿・丘吉尔有句名言,“不管战略多美妙,偶尔也得看看战果。”。
" However beautiful the strategy, you should occasionally look at the results.” is a famous saying by Sir Winston Churchill.
本期重症医学杂志刊发了 Stockmann 等人 (1) 的一项随机对照试验,执行严格,从结果看确实不错,研究细胞因子吸附治疗血管麻痹性休克 COVID-19 患者,一种关注度较高的治疗策略。(2)。
In this issue of Critical Care Medicine, Stockmann et al (1) did exactly that by looking at the result of a well-performed randomized controlled trial in which they investigated an intriguing strategy, namely the use of a cytokine adsorber, in patients with COVID-19 in vasoplegic shock (2).
与越来越流行的观点相反,在儿茶酚胺应用、病死率或其他次要结局(包括白细胞介素 - 6 (IL-6) 和 C - 反应蛋白 (CRP) 水平)上未见有任何差异。
In contrast to a growing popular belief, they neither showed any difference in the need for catecholamines nor in the mortality nor in other secondary outcomes, including interleukin (IL)-6 and C-reactive protein (CRP) levels.
2 年来,严重急性呼吸综合征冠状病毒 2 型 (SARSCoV-2) 引起的 COVID-19 对全球健康造成了严重影响。
For 2 years, the severe acute respiratory syndrome coronavirus 2 (SARSCoV-2) that causes the COVID-19 has had a serious impact on global health.
特别是疫情早期的那些院外患者,尚未施行疫苗接种预防也无药物治疗(如 remdesivir 或抗体介导策略),而重症患者治疗的手段基本上也就仅限于地塞米松 (3)。
Especially prior to the advent of prevention by vaccinations and pharmacologic treatment in the early phase of the disease in nonhospitalized patients like remdesivir or antibody-mediated strategies, the armamentarium for the treatment of critically ill patients was basically limited to dexamethasone (3).
在此背景下,在病程的不同阶段针对不同的靶点体外生命支持已经用于 COVID-19 重症患者的治疗。
On this background, extracorporeal treatments with different targets in nonidentical phases of the disease process have been explored in critically ill patients with COVID-19.
用新鲜冰冷冻血浆行治疗性血浆置换调整优化 von Willebrand 因子 / ADAMTS-13 之比[1]。
Therapeutic plasma exchange using fresh frozen plasma is applied to optimize the von Willebrand factor/a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 ratio (4).
在疾病的早期阶段使用病原吸附来减轻 SARSCov-2 病毒血症 (5,6)。
A pathogen adsorber is employed in the early phase of the disease to reduce SARSCov-2 viremia (5, 6).
最常用的干预措施旨在减少 COVID-19 患者的细胞因子风暴。
Among the most frequently used interventions are aimed to reduce the cytokine storm in COVID-19 patients.
2011 年,CytoSorb 在欧盟获得许可,作为一次性血液灌流设备,包含吸附聚合物磁珠,旨在清除分子量范围在 8-50 kDa 的物质。
In 2011, CytoSorb was licensed in the European Union as single-use hemoperfusion device containing adsorbent polymer beads designed to remove substances in the molecular weight range between 8 and 50 kDa.
促炎和抗炎细胞因子在该范围内。
Pro- and anti-inflammatory cytokines can be found in that range.
最近有学者提出,对紧急心脏手术的患者用 CytoSorb 清除替格瑞洛和利伐沙班 (7)。
Recently removal of ticagrelor and rivaroxaban by CytoSorb has been postulated in patients undergoing emergency heart operation (7).
2020 年 4 月 10 日,美国食品药品监督管理局批准 CytoSorb 在确诊的或即将发生呼吸衰竭的危重 COVID-19 患者可紧急使用。
On April 10, 2020, the U.S. Food and Drug Administration granted Emergency Use Authorization for CytoSorb use in critically ill COVID-19 patients with confirmed or imminent respiratory failure.
在单中心试点试验中,Stockmann et al (1) 入选了 50 例重症患者,为需要去甲肾上腺素大于 0.2µg/(kg・min) 维持平均动脉压≥65 mmHg、CRP 大于 100 mg/L 且需要肾脏替代治疗 (KRT) 的急性肾损伤 (AKI) 3 期的患者 (2)。
In the single-center pilot trial, Stockmann et al (1) enrolled 50 severely ill patients with need for norepinephrine greater than 0.2 µg/kg/min to maintain mean arterial pressure greater than or equal to 65 mm Hg, a CRP greater than 100 mg/L, and an acute kidney injury (AKI) stage 3 with need for kidney replacement therapy (KRT) (2).
两组至血管麻痹好转的中位时间(主要终点)和病死率(次要终点)均相似。
The median time to resolution of vasoplegia, the primary endpoint, was similar between both groups as was the secondary endpoint mortality rate.
此外,其他次要结局参数(炎症标志物、儿茶酚胺需求以及不良事件的类型和发生率)在治疗组间相似。
Furthermore, other secondary outcome parameters (inflammatory markers, catecholamine requirements, and the type and rates of adverse events) were similar between the groups.
由此,作者得出结论,在病情严重的 COVID-19 患者中,细胞因子吸附不能促进血管麻痹性休克的缓解。
Based on these data, the authors concluded that in severely ill COVID-19 patients, cytokine adsorption did not improve resolution of vasoplegic shock.
Stockmann 等 (1) 的研究中,细胞因子吸附未或成功的原因是什么?
What could have prevented the success of the intervention by cytokine adsorption in the study by Stockmann et al (1)?
细胞因子风暴的特征是循环细胞因子水平升高和免疫细胞过度活化,可由各种原因触发。一些作者认为,COVID-19 没有细胞因子风暴 (8),而是肝细胞生长因子和 C-X-C 基序趋化因子配体 13 失调 (9)。
Cytokine storm is characterized by elevated levels of circulating cytokines and immune-cell hyperactivation that can be triggered by various causes. Some authors argue that there is no cytokine storm in COVID-19 (8) but rather a dysregulation in hepatocyte growth factor and C-X-C motif chemokine ligand 13 (9).
事实上,重度 COVID-19 患者中促炎性细胞因子的全身浓度不像其他原因导致的急性呼吸窘迫综合征患者所报告的那样高。
Indeed, systemic concentrations of pro-inflammatory cytokines in patients with severe COVID-19 are not as high as has been reported in patients with other causes of acute respiratory distress syndrome.
Stockmann 等人的研究结果 (1) 与另一项随机对照研究的结果一致,该研究在脓毒性休克和多器官衰竭患者中进行,CytoSorb 清除 IL-6,但这种清除对全身 IL-6 水平没有影响 (10)。
The study results by Stockmann et al (1) are in line with the results of another randomized controlled study in patients with septic shock and multiple organ failure in which CytoSorb removed IL-6, but the removal had no effect on systemic IL-6-levels (10).
所以,像穿越加利利海猛烈的风暴出现神迹一样,因子风暴岂会轻易消退。
So calming the storm, as one of the miracles of Jesus in a fierce storm sailing the Sea of Galilee, seems to be a challenging endeavor.
其次,开始干预的时间可能太晚(指入院的时间以及疾病的状态)。
Second, intervention might have been initiated too late (referring to the time from admission as well as the state of the disease).
实际上,CytoSorb 自进入 ICU 至开始治疗的中位时间为 15 天,对照组为 10 天。
Indeed, median time since ICU admission to the start of the treatment was 15 days for CytoSorb and 10 days in the control group.
此外,入组患者不仅出现血管痉麻痹休克,还出现 AKI 和急性呼吸衰竭。
Further, the enrolled patients had not only vasoplegic shock but also AKI and acute respiratory failure.
所有患者均需要有创机械通气,其中几乎一半患者需要体外膜肺氧合 (ECMO) 治疗。
All patients required invasive mechanical ventilation and almost half of them required extracorporeal membrane oxygenation (ECMO) therapy.
然而,从实践上来看,11 例患者作者在休克 24 小时内开始治疗,另外 12 例患者是在 24 小时内开始治疗。
Yet from a practical point of view, the authors managed to start the treatment within 24 hours of shock in 11 patients and in 12 patients treatment was started after 24 hours.
Cox 回归分析显示,尽管患者数量有限,但在 24 小时内开始治疗并未获益。
Cox regression analysis revealed no benefit in starting the therapy within 24 hours, although the number of patients was limited.
联合 ECMO 开始治疗是否会得到不同的结果?
Could a concomitant start of treatment along with ECMO therapy have made a difference?
Supady et al (11) 该策略的最新数据未见获益。
The recent data by Supady et al (11) see no benefit of this strategy.
第三,已知 CytoSorb 可清除包括抗生素 (12) 和抗病毒药物(如 remdesivir (13))在内的药物,因此治疗组可能考虑抗感染药物剂量不足。这尤其有意义,因为半数患者在研究入选时微生物学培养也为阳性。
Third, CytoSorb is known to remove drugs including antibiotics (12) and antivirals like remdesivir (13), so the treatment group might have suffered from underdosing of anti-infective drugs. This is especially relevant as half of the patients also had positive microbiological cultures at the time of study inclusion.
尽管尚未获得治疗药物监测数据,但作者通过在 CytoSorb 组中每次更换过滤器时给予额外剂量的抗生素和瑞德西韦,来积极解决了这一问题。
Although therapeutic drug monitoring data are not available, the authors proactively addressed this point by giving an extra dose of antibiotics and remdesivir in the CytoSorb group with each filter change.
最后,与既往试验一样,CytoSorb 不是单一的体外治疗,而是与 KRT 联合使用,这也可能产生积极或消极的影响。
Last, as in previous trials, CytoSorb was not used as a stand-alone extracorporeal treatment but rather was used in combination with KRT, which might also have had a positive or negative impact.
这也将使 CytoSorb (14) 的未来研究难以解读为 KRT 本身,以及抗凝可能对患者结局产生影响 (15)。
This will also make future studies with CytoSorb (14) difficult to interpret as KRT per se, as well as the anticoagulation might have an impact on patient outcome (15).
在一项前瞻性、随机、开放标签研究中,Supady 等人 (11) 对 34 名接受 ECMO 治疗的 COVID-19 患者进行了研究,结果显示,无论是否使用 CytoSorb (11),在 72 小时内均出现 IL-6 中位数下降。
In a prospective, randomized, open-label study, Supady et al (11) investigated 34 COVID-19 patients with ECMO therapy and showed that the median IL-6 drop over 72 hours occurred regardless of the use of CytoSorb (11).
CytoSorb 组的 30 天病死率显著高于对照组 (11)。
Thirty-day mortality was significantly higher in the CytoSorb group as compared with the control group (11).
考虑到该研究,尽管在病死率上效能不足,但令人欣慰的是,Stockmann et al (1) 的研究显示无益但也未见潜在危害征象。
With that study in mind, although underpowered for mortality, it is comforting that the study by Stockmann et al (1) did show an absence of benefit and no sign of potential harm.
我们都希望不仅理解,而且可以通过降低促炎介质能很容易地解决炎症反应,但多项试验已证实这个想法是不对的。
Our collective hope that we not only understood but also could readily manipulate the inflammatory response by reducing pro-inflammatory mediators has been proven incorrect in several trials.
我们现在认识到炎症反应包括通过促炎和抗炎介质网络传播的复杂机制。
We now recognize the inflammatory response to include complex mechanisms propagated through networks of pro- and anti-inflammatory mediator.
已证实,仅解决这一网络的一小部分,例如使用单一或甚至几种抗炎治疗,已证明是无效的。
Addressing only a small part of that network, such as with a single or even several anti-inflammatory treatment, has proven ineffective.
同样,使用单一的非特异性吸附剂同样不太可能产生预期的有益作用。
Similarly, the use of a single nonspecific sorbent is equally unlikely to have a predictable salutary effect.
此外,分子中和或物理吸附可能会触发意外甚至是不良的后果。
Furthermore, molecular neutralization or physical adsorption may trigger unanticipated and even adverse consequences.
前瞻性对照试验设计之外,由于缺乏结果,应用 CytoSorb 的理由受到质疑。来自美国登记研究的数据 https://doi.org/10.3389/fmed.2021.773461 显示,1 年期内,接受 v-vECMO + CytoSorb 治疗的 52 例患者中,ICU30 天病死率为 17.3%(9/52),90 天病死率为 26.9%(14/52)。
Outside of the setting of controlled prospective trials, the rationale use of CytoSorb is questionable because of the lack of results. Data from a U.S. registry https://doi.org/10.3389/fmed.2021.773461 over a period of 1 year indicates in 52 patients receiving venovenous ECMO plus CytoSorb therapy an ICU mortality of 17.3% (9/52) on day 30 and 26.9% (14/52) on day 90.
CytoSorb 耐受性良好,未报告任何设备相关不良事件。
CytoSorb was well-tolerated without any devicerelated adverse events reported.
值得注意的是,还需要接受 KRT 的患者的比例仅为 21%。
It is of note the percentage of patients also requiring KRT was only 21%.
5.7% 的患者进行了治疗性血浆置换。
Therapeutic plasma exchange was used in 5.7% of the patients.
1921 年,丘吉尔的女儿玛丽戈尔德死于败血症。
Churchill’s daughter, Marigold, died of septicemia in 1921.
一百年后,我们的目标是在疫情大流行的健康危机中拯救尽可能多的生命。
One-hundred years later, we aim to save as many lives as possible amidst a pandemic health crisis.
这就能说使用 Cytosorb 这类未得到验证的设备是正确的吗?
Does this justify using untested devices like Cytosorb?
在大流行的早期阶段,这是一项还需要进一步探索的治疗选择。
In the early phase of the pandemic, it was among treatment options that needed to be explored.
不幸的是,2020 年在德国,多个 “病毒性肺炎” 研究的(至少)449 名患者中,仅有少数接受了 CytoSorb 治疗。
Unfortunately, we do only have a small number of the (at least) 449 patients that received CytoSorb in Germany in 2020 for “viral pneumonia” in studies.
纵观全球。许多其他体外操作情况也是如此。
The same holds true for many extracorporeal procedures worldwide.
更重要的是在感染性心内膜炎患者中使用 CytoSorb。
Even more relevant is the use of CytoSorb in patients with infective endocarditis.
感染性心内膜炎的心脏手术患者使用血液吸附预防血管舒张性休克的机制探索和疗效调查试验,是 CytoSorb 最大的(每组约 140 例患者)随机对照公共资助研究 (16)。
The Revealing Mechanisms and Investigating Efficiency Of Hemoadsorption for Prevention of Vasodilatory Shock in Cardiac Surgery Patients with Infective Endocarditis trial, the biggest (about 140 patients per arm) randomized controlled, publicly funded study with the CytoSorb (16).
该试验主要终点,改善序贯器官衰竭评估评分,和其他次要终点都未或成功。
The trial failed to reach its primary endpoint, an improvement of the Sequential Organ Failure Assessment score, as well as other secondary endpoints.
这是否会妨碍未来心血管外科医生使用该技术,以及保险公司的支付?
Will this keep cardiovascular surgeons from using it and insurance companies paying for it in the future?
在循证医学时代,我们需要新的策略,为新的干预措施和设备建立一个坚实的数据库。
In the era of evidence-based medicine, we need new strategies to build a solid database for new interventions and devices.
小公司需要有机会将新的(有时甚至是破坏性的)治疗方法推向市场。
Small companies need to get a chance to bring new—and at times disruptive therapies—to the market.
在理想的世界中,他们自己无需为做成随机对照、效力足够的试验来获得足够的收益,而应该与卫健系统和医疗人员合作。
In an ideal world, they should not need to generate enough revenue for controlled randomized, adequately powered trials themselves but should partner with healthcare systems and healthcare providers.
2020 年,德国保险公司支付了至少 6600 名患者 CytoSorb 治疗(有时是多个)的费用,但是没有将证据水平提高到现在的标准(图 1)。
In 2020, insurance companies in Germany payed for (sometimes multiple) CytoSorb treatments in at least 6,600 patients without increasing the evidence level to today’s standards (Fig. 1).
正如温斯顿・丘吉尔所言,无论提出的治疗策略背后的机制有多吸引人,干预措施仍然必须得到设计良好且具有充分效力的临床试验的阳性结果来证实。
To paraphrase Winston Churchill’s saying, no matter how intriguing the mechanisms behind a proposed therapeutic strategy might be, the intervention must still be substantiated by positive results of well designed and adequately powered clinical trials.
应当赞美 Stockmann 等人(1),因为他们所做的工作令人钦佩 —— 而那些对 Stockmann 等人(1)的结果提出质疑的人应该拿出令人信服的前瞻性随机对照研究证据。
Stockmann et al(1) should be commended for doing precisely that— and those challenging the results by Stockmann et al (1) should present compelling evidence from prospective randomized studies.
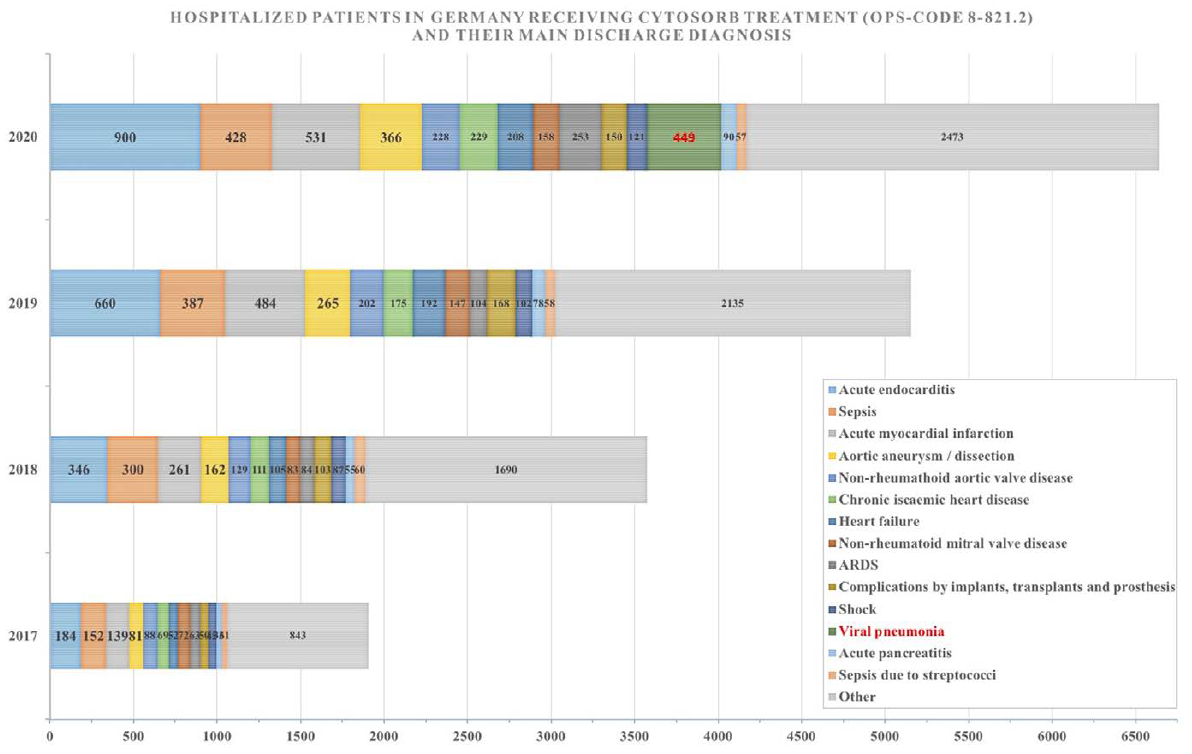
图 1. 2017 年至 2020 年间在德国至少接受过一次 Cytosorb 治疗的患者及其主要出院诊断 (Statistisches Bundesamt [Destatis],Wiesbaden,Germany)。尚不清楚每例患者的实际治疗次数。ARDS = 急性呼吸窘迫综合征,OPS-CODE = 手术和程序代码。
Figure 1. Patients that received at least one Cytosorb treatment in Germany from 2017 to 2020 as well as their primary discharge diagnosis (Statistisches Bundesamt [Destatis], Wiesbaden, Germany). The actual number of treatments per patient is not known. ARDS = acute respiratory distress syndrome, OPS-CODE = Operation and Procedure Code.
von Willebrand 因子:血管性血友病因子;ADAMTS13 是一种金属蛋白酶,主要在肝星状细胞中表达,特异性切割具有促血栓作用的大分子血管性血友病因子(von willebrand factor, VWF)多聚体。ADAMTS13 缺乏可导致超大分子 VWF 多聚体(UL-VWFM)持续存在于血管内,诱导血小板聚集,引发血栓性血小板减少性紫癜(TTP)。 ↩︎