
 脑血流自动调节的三个指数
脑血流自动调节的三个指数
#
# 通过心脏手术明确可识别自动调节下限的三个指标的阈值
Determining Thresholds for Three Indices of Autoregulation to Identify the Lower Limit of Autoregulation During Cardiac Surgery
Xiuyun Liu , Kei Akiyoshi , Mitsunori Nakano Mitsunori Nakano
Abstract 摘要
Objectives: Monitoring cerebral autoregulation may help identify the lower limit of autoregulation in individual patients. Mean arterial blood pressure below lower limit of autoregulation appears to be a risk factor for postoperative acute kidney injury. Cerebral autoregulation can be monitored in real time using correlation approaches. However, the precise thresholds for different cerebral autoregulation indexes that identify the lower limit of autoregulation are unknown. We identified thresholds for intact autoregulation in patients during cardiopulmonary bypass surgery and examined the relevance of these thresholds to postoperative acute kidney injury.
# 摘要
目的
监测脑血流自动调节有助于识别患者个体的自动调节下限。平均动脉压(MAP)低于自动调节下限可能是术后急性肾损伤(AKI)的危险因素。有相应的方法可实时监测脑血流自动调节。但是,识别脑血流自动调节下限的不同的脑血流自动调节指标的精确阈值尚不清楚。本研究在心肺旁路术中针对自动调节功能完好的患者来确定这些阈值,并检验这些阈值与术后 AKI 的相关性。
Design: A single-center retrospective analysis.
Setting: Tertiary academic medical center.
Patients: Data from 59 patients was used to determine precise cerebral autoregulation thresholds for identification of the lower limit of autoregulation. These thresholds were validated in a larger cohort of 226 patients.
患者
以 59 例患者的数据找到可识别自动调节下限的脑血流自动调节指标的精确阈值。在 226 例患者组成的更大队列中验证这些阈值。
Methods and main results: Invasive mean arterial blood pressure, cerebral blood flow velocities, regional cortical oxygen saturation, and total hemoglobin were recorded simultaneously. Three cerebral autoregulation indices were calculated, including mean flow index, cerebral oximetry index, and hemoglobin volume index. Cerebral autoregulation curves for the three indices were plotted, and thresholds for each index were used to generate threshold- and index-specific lower limit of autoregulations. A reference lower limit of autoregulation could be identified in 59 patients by plotting cerebral blood flow velocity against mean arterial blood pressure to generate gold-standard Lassen curves. The lower limit of autoregulations defined at each threshold were compared with the gold-standard lower limit of autoregulation determined from Lassen curves. The results identified the following thresholds: mean flow index (0.45), cerebral oximetry index (0.35), and hemoglobin volume index (0.3). We then calculated the product of magnitude and duration of mean arterial blood pressure less than lower limit of autoregulation in a larger cohort of 226 patients. When using the lower limit of autoregulations identified by the optimal thresholds above, mean arterial blood pressure less than lower limit of autoregulation was greater in patients with acute kidney injury than in those without acute kidney injury.
方法和结果
同时记录有创 MAP、脑血流速、区域皮质氧饱和度 (rScO2),和血红蛋白总数。计算三个脑血流自动调节指标,包括平均血流速度指数、脑血氧指数以及血红蛋白容积指数。绘制三个指数的脑血流自动调节曲线,并用每个指数的阈值生成具体自动调节下限的阈值和指数。通过绘制 59 例患者的脑血流速和 MAP 得到金标准 Lassen 曲线,找到一个自动调节下限的参考值。每个阈值确定一个自动调节下限,与 Lassen 曲线确定的自动调节下限金标准比较。以下结果为确定的阈值:平均血流速度指数(0.45),脑血氧指数(0.35),血红蛋白容积指数(0.3)。随后对较大队列的 226 患者计算 MAP 低于自动调节下限的数值和持续时间的乘积。当采用上述最佳阈值确定的自动调节下限时,平均动脉压低于自动调节下限的 AKI 患者比非 AKI 患者更多。
Conclusions: This study identified thresholds of intact and impaired cerebral autoregulation for three indices and showed that mean arterial blood pressure below lower limit of autoregulation is a risk factor for acute kidney injury after cardiac surgery.
结论
该研究确定了脑血流自动调节完好和受损的三个指标的阈值,证明平均动脉压低于自动调节下限时心脏术后急性肾损伤的危险因素。
内容摘录
# 背景
| 译文 | 原文 |
|---|---|
| 背景 | BACKGROUND |
| 脑血流自动调节(Cerebral autoregulation ,CA)是指大脑在平均动脉压较大范围波动时维持脑血流(cerebral blood flow ,CBF)相对恒定的能力。 | Cerebral autoregulation (CA) refers to the ability of the brain to maintain relatively constant cerebral blood flow (CBF) over wide changes in mean arterial blood pressure (MAP) . |
| MAP 低于脑血流自动调节下限(LLA)时,代偿机制不足,CBF 就会随 MAP 一同下降。 | However, when MAP decreases below the lower limit of autoregulation (LLA), compensatory mechanisms become inadequate, and CBF decreases monotonically with MAP. |
| 在神经重症,对于神经急危患者,目标 MAP 在恰当的范围内至关重要,血压纠正过度或不足都会增加病死率和并发症。 | In the neurocritical care unit, targeting MAP at the correct range in patients with neurologic emergencies is critical, as both over- and under correction of blood pressure are associated with increased morbidity and mortality. |
| MAP 低于 LLA 的程度与主要并发症和病死率,AKI 以及谵妄有关。 | Maintaining MAP above LLA may be especially important during CPB surgery, as studies have suggested that the extent of MAP below the LLA is associated with major morbidity and mortality, acute kidney injury (AKI), and delirium. |
| 通过比较脑血流(CBF)随血压变化的自动改变可实时评估重症患者的脑血流自动调节(CA)。 | The CA of critically ill patients can be assessed in real time by comparing spontaneous CBF changes in response to changes in MAP. |
| 采用多模监测,根据 CBF 的变化和 MAP 的变化计算的相关系数波动在 -1(自动调节完好) 到 1 (自动调节受损)之间。 | Using multimodal monitoring, a moving correlation coefficient is calculated between changes in CBF and changes in MAP. This correlation coefficient is termed the “index of autoregulation” and can vary between –1 (intact autoregulation) and 1 (impaired autoregulation). |
| 代替脑血流监测的自动调节指标有:平均血流指数(Mx,据经颅多普勒(TCD)血流计算而来),脑血氧指数(COx,据皮质局部氧饱和度计算而来),血蛋白容积指数(HVx,据局部血红蛋白总数(rTHb)计算而来)。 | Based on the surrogate of CBF that is monitored, several indices of autoregulation have been described, including the mean flow index (Mx, derived from transcranial Doppler [TCD] flow), cerebral oximetry index (COx, derived from regional cortical oxygen saturation [rSo2 ]), and hemoglobin volume index (HVx, derived from regional total hemoglobin [rTHb]) . |
# 材料与方法
| 译文 | 原文 |
|---|---|
| 材料与方法 | MATERIALS AND METHODS |
| 患者 | Patients |
| 纳入约翰霍普金斯医院 2017-1-4 至 2019-8-23 行 CPB 手术的患者。 | Patients undergoing CPB surgery at Johns Hopkins Hospital (Baltimore, MD) were enrolled between January 4, 2017, and August 23, 2019. |
| 入选标准: 18 岁以上,冠脉旁路移植、瓣膜、主动脉或心肌切除单独或联合手术 | Patients were in-cluded if they were greater than 18 years old and under-going isolated or combined cardiac artery bypass graft, valve, aortic, or myectomy surgery. |
| 排除标准: 心脏或肺移植,装有心室辅助装备,已有肾脏疾病,无 TCD 检查声窗。 | Exclusion criteria were lung or heart transplant, insertion of a ventricular assist device, or pre-existing kidney disease. Patients without windows for TCD analysis were excluded. |
| 共纳入 226 例,亚组中 59 例获得 Lassen 曲线,据此得到识别 LLA 的自动调节指数的阈值。然后在全部 226 例患者队列中验证这些阈值与 AKI 的关系。 | Of the 226 patients enrolled, a subset of these patients (n = 59) had Lassen curves, and their data were used in the primary analysis to derive thresholds of autoregulation for identification of the LLA. The full cohort of 226 patients was then used to validate these thresholds in relation to AKI. |
| 获取信号 | Signal Acquisition |
| 通过 TCD 使用 2.5-MHz 探头监测双侧大脑中动脉获得脑血流速(CBFV)。 | CBF velocity (CBFV) was monitored through bilateral TCD of the middle cerebral arteries, MCAs (Doppler Box; DWL, Singen, Germany), using 2.5-MHz probes. |
| 患者前额防治两个近红外光谱(NIRS)电极持续监测 rTHB 和 rSo2。 | Two near-infrared spectroscopy (NIRS) probes (Covidien, Boulder, CO) were placed on the patient’s forehead to monitor rTHb and rSo2. The data were re-corded continuously in the operating room. |
| 有创监测桡或股动脉获得 MAP。使用软件同步记录,手工删除吸痰、冲管、传感器问题导致的伪差。 | MAP was monitored invasively through the radial or femoral artery. All signals were sampled at 128 Hz and recorded synchronously using ICM+ software through an analog-to-digital converter or digitally, directly from GE Solar monitors . Artifacts introduced by tracheal suction-ing, arterial catheter flushing, or transducer malfunction were removed manually. |
| 术中处置(略) | Perioperative Care |
| 根据金标准“Lassen 曲线”确定LLA | Defining the LLA With the Gold-Standard “Lassen Curve” |
| 用三个不同的自动调节指数定义 LLA | Defining the LLA Using Three Different Indices of Autoregulation |
|---|---|
| 计算三个不同的自动调节指数:Mx、HVx 和 COx。 | Three different indices of autoregulation were calculated: Mx, HVx, and COx. |
| 在 300 秒的数据窗口内,计算 10 秒钟 MAP 和 TCD CBFV 的均值的移动皮尔森相关系数得到 Mx。 | Mx was calculated as a moving Pearson correlation coefficient between 10-second averages of MAP and TCD CBFV, using a 300-second data window |
| 同样,COx 通过 10 秒钟 MAP 和 NIRS rSO2 均值的移动皮尔森相关系数计算, | Similarly, COx was calculated as a moving Pearson correlation coefficient between 10-second averages of MAP and NIRS rSO2, |
| HVx 为 10 秒钟 MAP 和 NIRS rTHb 的系数。 | and HVx was calculated as the correlation between 10-second averages of MAP and NIRS rTHb. |
| 由于正常 MAP 和 CBF 呈负相关或不相关,所以 Mx,,Cox,,或 HVx 的值为负或接近 0 代表自动调节具有功能。 | Functional autoregulation is indicated by negative or near-zero Mx, Cox, or HVx values because MAP and CBF are negatively or not correlated. |
| Mx,COx,或 HVX 的值较高带都曾 CA 受损(此时 CBF 与 MAP 相关) | Impaired CA is indicated by high Mx, Cox, or HVx (CBF and MAP are correlated) . |
| 要用 CA 相关的基本变量定义 LLA,故绘制 Mx (或 COx 或 HVx)和 MAP(以 5 mmHg 为间隔)的 “U 型” 拟合算法曲线。 | To define the LLA using CA correlation-based variables, we plotted Mx (or Cox or HVx) against MAP in 5 mm Hg bins and applied a “U-shape” curve fitting algorithm . |
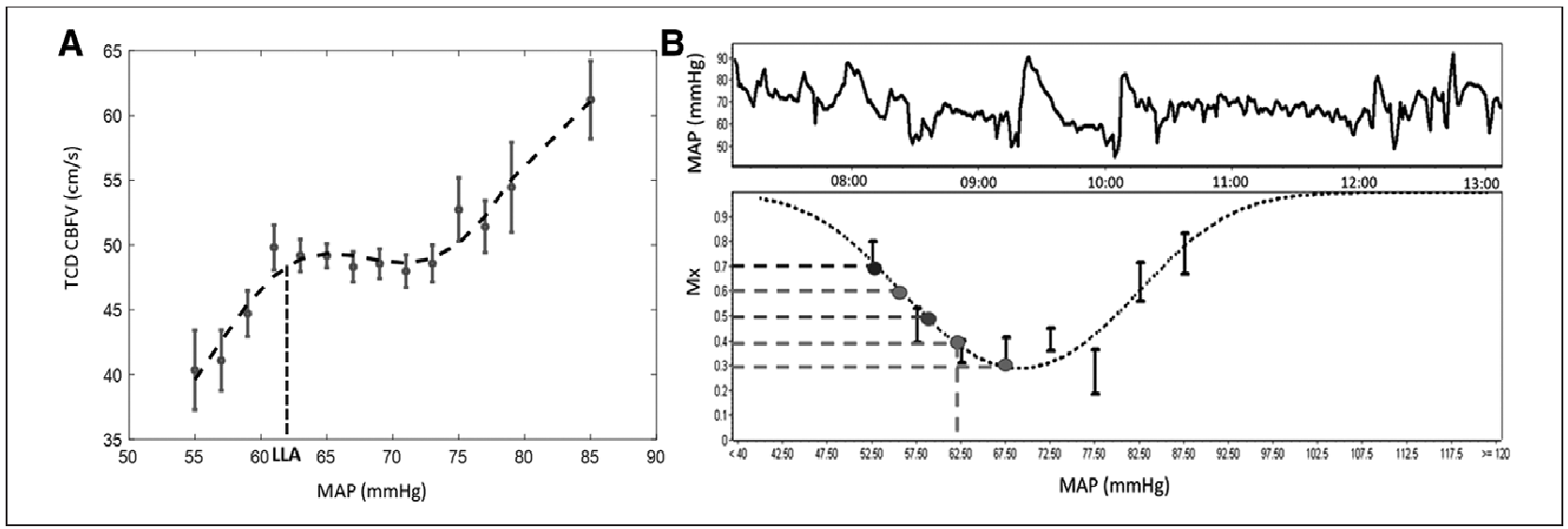
| 软件采用不同的阈值(0.1-0.9 之间,间隔 0.05)画出阈值的水平直线来定义各个 CA 阈值的 LLAs,图 1B。 | We used different cutoffs to identify LLAs at different CA thresholds (ranging from 0.1 to 0.9 at intervals of 0.05) by drawing a straight horizontal line at the cutoff value using ICM+ software as shown in Figure 1B. |
| 直线和 U 型曲线相交所对应的 X 轴上的点定义为 LLA(图 1B),如果没有相交视为缺失。 | The x coordinate of the point at which the straight line meets the U-shaped curve was defined as the LLA (Fig 1B) or treated as missing in the absence of an intersection. |
| 小于 LLA 的 MAP 的曲线下面积 | Area Under the Curve of MAP Below LLA |
|---|---|
| 为了定量衡量 LLA 和患者预后之间的关系,心脏术中 MAP 低于 LLA 的程度在血压数值和持续时间(hr)上通过计算压力差 - 时间乘积的曲线下面积来表示。 | To quantify the relationship between LLA and patient outcome, we expressed the extent of MAP less than LLA during the cardiac surgery procedure in terms of magnitude (mm Hg) and duration (hr) by calculating the area under the curve of the product of magnitude versus time (AUC): |
| 其中 ΔTime 为时间,Magnitudei为每个样本 MAP 低于 LLA 的差值。(以低于 LLA 的 MAP 的压力差 - 时间乘积来衡量 MAP 低于 LLA 的程度。) | where ΔTime is the time, and Magnitudei is the individual sample values for the magnitude of MAP deviation below the LLA. (We refer to this product of magnitude-time dose of MAP less than LLA as the extent of MAP below LLA.) |
| 急性肾损伤 | AKI |
|---|---|
| 以术后 2 天血肌酐(SCr)与术前基线相比变化最大的值,采用急性肾损伤网络的标准(SCr 升高>1.5 倍或 48 小时内急性升高 > 0.3 mg/dL)来定义 AKI。 | AKI was defined by comparing the maximal change in serum creatinine (SCr) in the first 2 postoperative days with baseline values measured before surgery using the Acute Kidney Injury Network criteria (increase in the ratio of SCr > 1.5 or acute rise in SCr > 0.3 mg/dL within 48 hr) . |
| 统计分析 | Statistical Analysis |
|---|---|
| 统计分析采用 Matlab(版本 R2019B)和 SPSS(版本 25.0)软件包。 | Statistical analyses were calculated with Matlab soft-ware (version R2019B, MathWorks, Natick, MA) and SPSS (Version 25.0, IBM, Armonk, NY). |
| 患者特征和围术期特征采用 Fisher 精确检验、Student t 检验和曼 - 惠特尼 U 检验进行比较。 | Patient and perioperative characteristics were compared by Fisher exact tests, Student t tests, and Mann-Whitney U tests. |
| 计算两种 LLA 间差值的布兰德 - 奥特曼散点图(B-A 图)和均方根(RMS),来分析 LLA_Laseen 和脑血流自动调节参数定义的 LLA 的关系。 | To analyze the relationship between LLA_Lassen and LLA defined by CA parameters, we calculated Bland-Altman plots and root-mean square (RMS) of the difference between the two types of LLA. |
| 均方根(RMS)的计算公式为 | The RMS was calculated as |
| 布兰德 - 奥特曼均差表示差值的中心(实际值常在均值的一边),并只对位置敏感,而均方根是差值平方和的数学平均数的平方根,对位置和大小均敏感。 | The mean difference in Bland-Altman indicates the “center” of the difference (the actual values are to be found on either side of the mean) and is only sensitive to location, whereas the RMS is the square root of the arithmetic mean of the squares of the difference, and it is sensitive to both location and scale. |
To validate the cutoffs obtained for the three CA variables (Mx, HVx, and COx), we categorized the patients into groups with/without AKI after the sur-gery. The mean extent of MAP less than LLA at differ-ent cutoffs was calculated for each patient with an LLA; otherwise, the extent was treated as missing. Then the mean extent of MAP less than LLA of patients with and without AKI was compared by the nonparametric Mann-Whitney U test. Unadjusted logistic regres-sion and multivariable logistic regression adjusted by age, operation duration, logistic European System for Cardiac Operative Risk Evaluation, diabetes, con-gestive heart failure, current smoker, aspirin use, hy-pertension history, and preoperative pulse pressure (potentially confounding variables based on prior lit-erature [11]) were used to examine the association of mean extent of ABP less than LLA with AKI. For all