连续监测脑血管压力反应性可以确定创伤性脑损伤患者的最佳脑灌注压力
Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury
Steiner LA, Czosnyka M, Piechnik SK, et al. Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Crit Care Med. 2002;30(4):733-738. doi:10.1097/00003246-200204000-00002
DeepL 翻译 + 人工校对 摘要
Objectives : To define optimal cerebral perfusion pressure (CPPOPT) in individual head-injured patients using continuous monitoring of cerebrovascular pressure reactivity. To test the hypothesis that patients with poor outcome were managed at a cerebral perfusion pressure (CPP) differing more from their CPPOPT than were patients with good outcome.
目的:通过对脑血管压力反应性的连续监测,确定脑外伤患者个体的最佳脑灌注压(CPPOPT)。检验结果不佳的患者的脑灌注压 (CPP) 与结果良好的患者的 CPPOPT 相差较大的假设。
Design : Retrospective analysis of prospectively collected data.
Setting : Neurosciences critical care unit of a university hospital.
Patients : A total of 114 head-injured patients admitted between January 1997 and August 2000 with continuous monitoring of mean arterial blood pressure (MAP) and intracranial pressure (ICP).
患者: 1997 年 1 月至 2000 年 8 月期间入院的共 114 名脑外伤的病人,对平均动脉血压(MAP)和颅内压(ICP)进行连续监测。
Measurements and Main Results : MAP, ICP, and CPP were continuously recorded and a pressure reactivity index (PRx) was calculated online. PRx is the moving correlation coefficient recorded over 4-min periods between averaged values (6-sec periods) of MAP and ICP representing cerebrovascular pressure reactivity. When cerebrovascular reactivity is intact, PRx has negative or zero values, otherwise PRx is positive. Outcome was assessed at 6 months using the Glasgow Outcome Scale. A total of 13,633 hrs of data were recorded. CPPOPT was defined as the CPP where PRx reaches its minimum value when plotted against CPP. Identification of CPPOPT was possible in 68 patients (60%). In 22 patients (27%), CPPOPT was not found because it presumably lay outside the studied range of CPP. Patients' outcome correlated with the difference between CPP and CPPOPT for patients who were managed on average below CPPOPT (r = .53, p < .001) and for patients whose mean CPP was above CPPOPT (r = -.40, p < .05).
测量和主要结果:连续记录 MAP、ICP 和 CPP,并在线计算压力反应性指数(PRx)。PRx 是 4 分钟内记录的 MAP 和 ICP 的平均值(每间隔 6 秒计算一次平均值,4 分钟有 40 组数据)之间的移动相关系数,代表脑血管压力反应性。当脑血管反应性完整时,PRx 为负值或零,否则 PRx 为正值。6 个月时使用格拉斯哥结果量表评估结果。总共记录了 13,633 小时的数据。CPPOPT 被确定为 PRx 在与 CPP 作图时达到最低值的 CPP。68 名患者(60%)可以确定 CPPOPT。22 名患者(27%)没有找到 CPPOPT,因为它可能在研究的 CPP 范围之外。对于平均管理水平低于 CPPOPT 的患者(r = .53,p < .001)和平均 CPP 高于 CPPOPT 的患者(r = -.40,p < .05),患者预后与 CPP 和 CPPOPT 之间的差异相关。
Conclusions : CPPOPT could be identified in a majority of patients. Patients with a mean CPP close to CPPOPT were more likely to have a favorable outcome than those whose mean CPP was more different from CPPOPT. We propose use of the criterion of minimal achievable PRx to guide future trials of CPP oriented treatment in head injured patients.
结论:大多数患者的 CPPOPT 可以被识别。平均 CPP 接近 CPPOPT 的患者比平均 CPP 与 CPPOPT 相差较大的患者更有可能获得良好的预后。对未来实施的脑外伤患者 CPP 导向治疗试验,我们建议使用可用的最小 PRx 标准来指导。
序言
Cerebrovascular pressure reactivity is defined as the ability of vascular smooth muscle to respond to changes in transmural pressure. This is one of the key mechanisms responsible for autoregulation of cerebral blood flow ([1]). However, the two expressions should not be used synonymously as vasodilatation reaches its maximum at arterial pressures below the lower threshold for constant cerebral blood flow ([2]).
脑血管压力反应性被定义为血管平滑肌对跨膜压力变化的反应能力。这是负责脑血流自动调节的关键机制之一([1])。然而,这两个词不应作为同义词使用,因为低于恒定脑血流的下限所对应的血压时血管达到了最大限度的扩张([2])。
Cerebrovascular pressure reactivity can be determined by observing the response of intracranial pressure (ICP) to changes in mean arterial blood pressure (MAP). If pressure reactivity is intact, a rise in MAP will lead within 5-15 secs to a vasoconstriction with reduction of cerebral blood volume and ICP will decrease. If it is defective, cerebral blood volume will increase passively and ICP will rise. The opposite applies to a reduction in MAP ([3]). These rules do not apply in all instances, for example, when the change in MAP is very fast or large ([4]). However, in the majority of clinical situations where slow and not too pronounced changes in MAP are observed they may be safely used. Where the pressure-volume compensatory reserve of the brain is reduced, for example, as after head injury ([5]), the relationship between MAP and ICP will be accentuated. Taking advantage of this observation, cerebrovascular pressure reactivity can be measured continuously without the artificial manipulation of MAP. Observations of spontaneous fluctuations in MAP and ICP have been reported by several authors ([6, 7]), who agreed that a negative correlation between MAP and ICP could be interpreted as good vasoreactivity, whereas a positive correlation was associated with disturbed vasoreactivity. Computer-aided methods with which to determine cerebrovascular pressure reactivity were introduced by two different groups ([8, 9]). They proposed moving coherence or correlation indices to express the relationship between spontaneous slow (20 secs to 2 mins) waves of MAP and ICP. The method developed at Cambridge ([9]) calculates a pressure reactivity index (PRx) as a correlation coefficient having values in the range between -1 and + 1. A negative or zero value reflects a normally reactive vascular bed whereas positive values reflect passive, nonreactive vessels. Moreover, one of the strengths of this global index of cerebrovascular pressure reactivity is that it reflects graded loss of autoregulation not just "present or absent."
脑血管压力反应性可以通过观察颅内压(ICP)对平均动脉血压(MAP)变化的反应来确定。如果压力反应性是完整的,MAP 的上升将在 5-15 秒内导致血管收缩,脑血容量减少,ICP 将下降。若受损,脑血容量将被动增加,ICP 将上升。MAP 的降低则相反([3])。这些规律并非在所有情况下都存在,例如,当 MAP 的变化非常快或很大的情况([4])。然而,在大多数临床情况下,如果观察到 MAP 缓慢且不太明显的变化,可以安全地使用这些规则。当大脑的压力 - 容积代偿储备减少时,例如脑外伤后([5]),MAP 和 ICP 之间的关系就会加强。利用这一观察,可以连续测量脑血管压力反应性,而不需要人为地操纵 MAP。一些作者([6, 7])报告了对 MAP 和 ICP 自发波动的观察,他们一致认为 MAP 和 ICP 之间的负相关可以解释为血管反应性良好,而正相关则与血管反应性紊乱有关。两个不同的小组([8, 9])提出了计算机辅助方法,以确定脑血管压力反应性。他们提出了移动相干性或相关指数来表达 MAP 和 ICP 的自发慢波(20 秒至 2 分钟)之间的关系。剑桥大学开发的方法([9])将压力反应性指数(PRx)计算为一个相关系数,其值在 - 1 和 + 1 之间。负值或零值反映了正常反应性的血管床,而正值反映了被动的、无反应的血管。此外,这种脑血管压力反应性的总体指数的优点之一是它反映了自动调节丧失的等级程度,而不仅仅是 "有或无"。
Previous studies have shown a significant correlation between PRx and outcome after head injury ([9, 10]), which included a time-dependent element: if PRx persisted above 0.2 for more than 6 hrs, this was usually associated with fatal outcome ([10]). PRx has been shown to react dynamically to changes in cerebral perfusion pressure (CPP) and it has been possible to define lower breakpoints of autoregulation in some patients ([10]).
以前的研究显示,PRx 与脑外伤后的结果有明显的相关性([9, 10]),其中包括时间依赖因素:如果 PRx 持续在 0.2 以上超过 6 小时,这通常与致命性预后有关([10])。PRx 已被证明对脑灌注压(CPP)的变化存在动态反应,并且有可能在一些病人中指定更低的自动调节折点([10])。
We hypothesized that, because of the dynamic relationship between CPP and PRx, it would be possible to define a CPP at which PRx reaches its optimal (lowest) value in an individual patient (CPPOPT). Because PRx correlated with outcome, we further hypothesized that patients whose average CPP during intensive care treatment had been distinctly different from CPPOPT had a less favorable outcome than patients whose average CPP had been in the proximity of CPPOPT.
我们假设,由于 CPP 和 PRx 之间的动态关系,有可能确定一个 CPP,在这个 CPP 上,PRx 达到病人个体的最佳(最低)值(CPPOPT)。由于 PRx 与预后相关,我们进一步假设,在重症医学科治疗期间平均 CPP 与 CPPOPT 明显不同的患者,其预后不如平均 CPP 接近 CPPOPT 的患者。
材料和方法
患者
We studied 114 head-injured patients who were admitted to the Neuroscience Critical Care Unit of Addenbrooke's Hospital's in Cambridge between January 1997 and August 2000 for whom outcome data were available. Their ages ranged from 14 to 77 yrs. The Glasgow Coma Score (GCS) at admission ranged from 3 to 14. Initial computed tomography (CT) showed epidural hematomas in 14 patients (12%), which were evacuated surgically in 12 patients. Subdural hematomas were initially present in 24 patients (21%) and developed in 3 patients later on. Thirteen of the subdural hematomas were evacuated surgically. Further, three patients had decompressive craniectomy or lobectomy. Extensive traumatic subarachnoid hemorrhage was present in a further 17% and intracranial hemorrhage in 10% of the patients. Outcomes and baseline data are presented in [Table 1].
我们研究了 1997 年 1 月至 2000 年 8 月期间入住剑桥大学阿登布鲁克医院神经科学重症医学科的 114 名脑外伤的病人,都有预后数据。年龄从 14 岁到 77 岁不等。入院时的格拉斯哥昏迷评分(GCS)从 3 到 14 不等。最初的计算机断层扫描(CT)显示 14 名患者(12%)有硬膜外血肿,其中 12 名患者通过手术清除。24 名患者(21%)最初出现硬膜下血肿,3 名患者后来发展为硬膜下血肿。其中 13 名硬膜下血肿通过手术清除。此外,3 名患者进行了减压性颅骨切除术或脑叶切除术。还有 17% 的患者出现了广泛的创伤性蛛网膜下腔出血,10% 的患者出现了颅内出血。结果和基线数据列于 [表 1]。
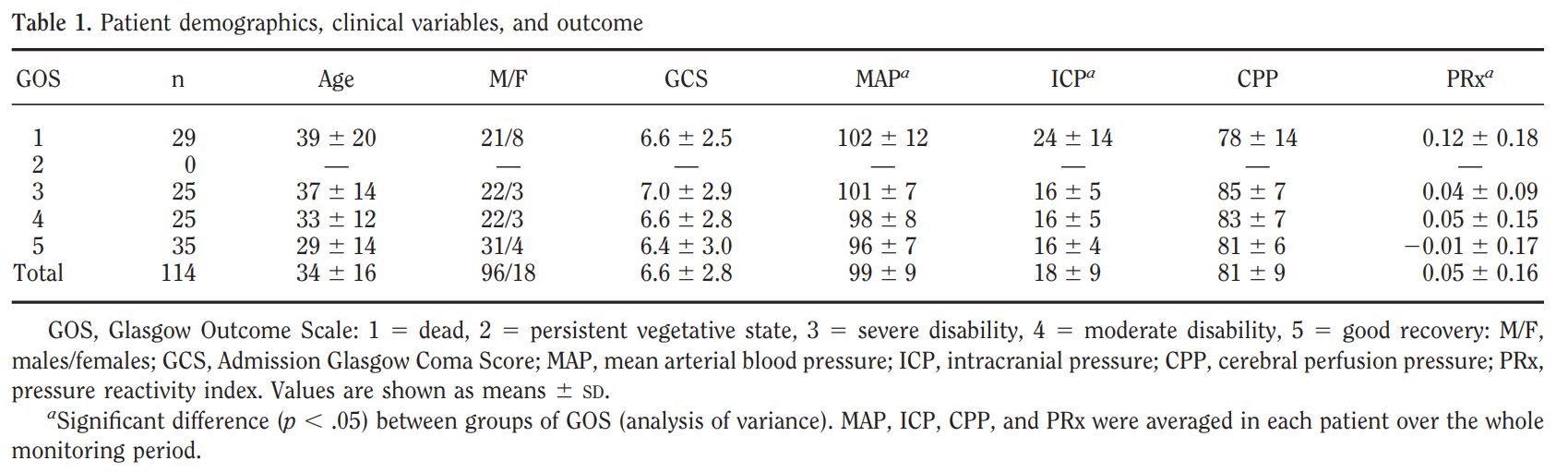
Table 1. Patient demographics, clinical variables, and outcome
GOS, Glasgow Outcome Scale: 1 = dead, 2 = persistent vegetative state, 3 = severe disability, 4 = moderate disability, 5 = good recovery: M/F, males/females; GCS, Admission Glasgow Coma Score; MAP, mean arterial blood pressure; ICP, intracranial pressure; CPP, cerebral perfusion pressure; PRx, pressure reactivity index. Values are shown as means +/- sd.
a Significant difference (p < .05) between groups of GOS (analysis of variance). MAP, ICP, CPP, and PRx were averaged in each patient over the whole monitoring period.
表 1. 患者人口统计学、临床变量和预后
GOS,格拉斯哥结果量表。1 = 死亡,2 = 持续植物状态,3 = 严重残疾,4 = 中度残疾,5 = 恢复良好。M/F,男性 / 女性;GCS,入院格拉斯哥昏迷评分;MAP,平均动脉血压;ICP,颅内压;CPP,脑灌注压;PRx,压力反应性指数。数值显示为平均值 +/-sd.
a 各组 GOS 之间有显著差异(P < .05)(方差分析)。每个病人在整个监测期间的 MAP、ICP、CPP 和 PRx 均为平均数。
All patients were initially sedated with propofol and artificially ventilated. Ventilators were adjusted to achieve a Paco2 of 30-35 torr (4.0-4.5 kPa). Analgesia was provided with fentanyl and atracurium was used for neuromuscular blockade in all patients. A CPP-oriented treatment strategy was used with a target CPP of at least 70 mm Hg. Volume expansion, dopamine, and/or norepinephrine were used at the discretion of the responsible physician to achieve this. ICP above 20 mm Hg was treated with boluses of mannitol (2 mg/kg). The patients were nursed flat and kept normothermic.
所有患者最初都用丙泊酚镇静,并进行人工呼吸。调整呼吸机以达到 30-35torr(4.0-4.5 kPa)的 Paco2。用芬太尼进行镇痛,并在所有患者中使用阿曲库铵进行神经肌肉阻断。采用以 CPP 为导向的治疗策略,目标 CPP 至少为 70mmHg。为了达到这个目标,负责的医生会酌情使用容量扩张、多巴胺和 / 或去甲肾上腺素。ICP 超过 20 毫米汞柱时,使用甘露醇(2 mg/kg)进行治疗。对患者进行平卧护理并保持正常体温。
数据采集和处理
As part of standard clinical practice, MAP was monitored directly from the radial artery using a standard pressure monitoring kit (Baxter Healthcare, CardioVascular Group, Irvine, CA). ICP was monitored continuously with an intraparenchymal transducer (Camino Direct Pressure Monitor, Camino Laboratories, San Diego, CA, or Codman MicroSensors ICP Transducer, Codman & Shurtleff, Raynham, MA).
作为标准临床实践的一部分,使用标准压力监测套件(Baxter Healthcare, CardioVascular Group, Irvine, CA)直接从桡动脉监测 MAP。ICP 是用脑膜内传感器(Camino 直接压力监测器,Camino 实验室,加州圣地亚哥,或 Codman MicroSensors ICP 传感器,Codman & Shurtleff,马萨诸塞州雷纳姆)连续监测的。
Analog output from all bedside monitors was processed through an analog-to-digital converter (DT 2814; Data Translation, Marlboro, MA) and stored on a portable computer (Amstrad ALT 386 SX; AMSTRAD, Kowloon, Hong Kong) using software developed in-house ([11]). Sampling frequency was 30 Hz. Time-averaged means for arterial blood pressure, ICP, and CPP (CPP = MAP - ICP) were calculated and stored every minute. For calculation of PRx, average values of MAP and ICP were calculated for 6-sec intervals using waveform time integration. PRx was calculated every 60 secs as a moving linear (Pearson's) correlation coefficient between the last 40 consecutive 6-sec averages of MAP and ICP as described previously ([9]). An example of a raw data plot of a single patient is shown in [Figure 1].
所有床边监护仪的模拟输出通过模数转换器(DT 2814; Data Translation, Marlboro, MA)进行处理,并使用内部开发的软件([11])存储在一台便携式计算机(Amstrad ALT 386 SX; AMSTRAD, Kowloon, Hong Kong)上。采样频率为 30 Hz。每分钟计算并储存动脉血压、ICP 和 CPP(CPP = MAP - ICP)的时间平均数。对于 PRx 的计算,使用波形时间积分计算 6 秒间隔的 MAP 和 ICP 的平均值。如前所述([9]),PRx 每 60 秒计算一次,作为 MAP 和 ICP 最后 40 个连续 6 秒平均值之间的移动线性(Pearson)相关系数。一个单一病人的原始数据图的例子显示在 [图 1]。
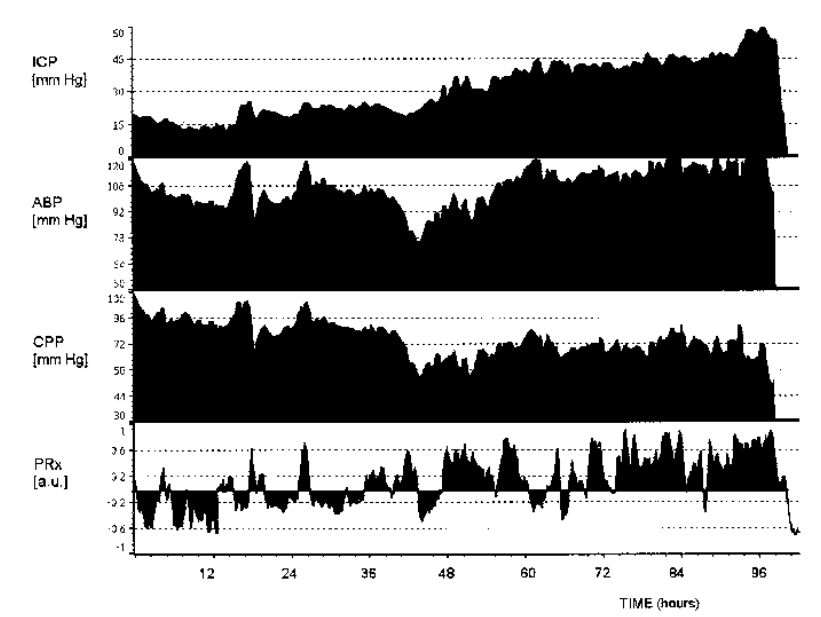
Figure 1. Standard output as obtained by our bedside monitoring system (laptop computer) after artifact removal. The traces represent the 96-hr monitoring period of the same patient as shown in [Figure 2c]. ICP, intracranial pressure;ABP, mean arterial blood pressure;CPP, cerebral perfusion pressure;PRx, pressure reactivity index;a.u., arbitrary units. This plot illustrates the progressive disturbance of cerebrovascular pressure reactivity in a patient who died because of refractory intracranial pressure: 0-36 hrs: reactivity on average good with the exception of two episodes of high ABP (>110 mm Hg); 36-72 hrs: unstable ABP with CPP frequently <70 mm Hg and protracted episodes of disturbed reactivity; 72-96 hrs: almost permanent loss of reactivity associated with high ICP.
图 1. 我们的床旁监测系统(笔记本电脑)在去除伪影后获得的标准输出。这些痕迹代表了 [图 2c] 中所示的同一病人的 96 小时监测期。ICP,颅内压;ABP,平均动脉血压;CPP,脑灌注压;PRx,压力反应性指数;a.u.,任意单位。该图说明了一名因难治性颅内压而死亡的病人的脑血管压力反应性的逐渐紊乱:0-36 小时:除了两次高 ABP(>110 毫米汞柱)外,反应性平均良好;36-72 小时:ABP 不稳定,CPP 经常 < 70 毫米汞柱,反应性紊乱发作时间延长;72-96 小时:与高 ICP 相关的反应性几乎永久丧失。
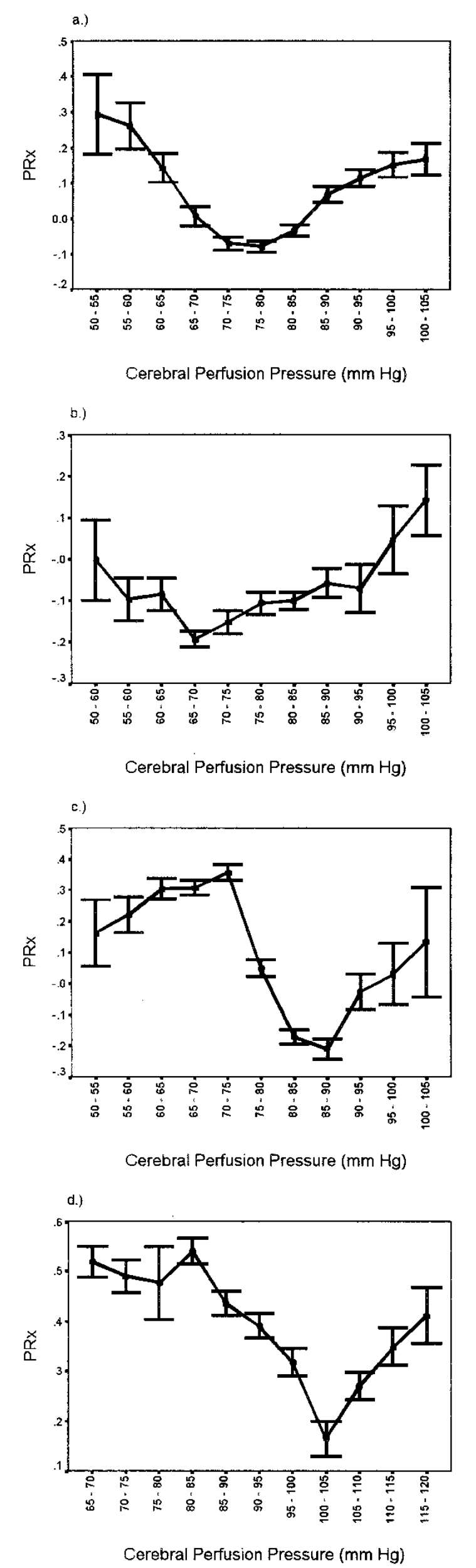
Figure 2. Examples of pressure reactivity index (PRx) vs. cerebral perfusion pressure (CPP) plots that allow determination of optimal cerebral perfusion pressure (CPPOPT) in individual patients. (a) Good Recovery, CPP - CPPOPT = 3 mm Hg. (b) Moderate disability, CPP - CPPOPT = 7 mm Hg. (c) Dead, CPP - CPPOPT = -16 mm Hg. (d) Dead, CPP - CPPOPT = -10 mm Hg. Error bars represent 95% confidence intervals.
图 2. 压力反应性指数(PRx)与脑灌注压(CPP)图例,可以确定病人个体的最佳脑灌注压(CPPOPT)。(a) 恢复良好,CPP-CPPOPT=3mmHg。(b) 中度残疾,CPP-CPPOPT = 7 mm Hg。(c) 死亡,CPP-CPPOPT = -16 mm Hg。(d) 死亡,CPP-CPPOPT = -10 mm Hg。误差条代表 95% 的置信区间。
This kind of MAP/ICP monitoring is standard clinical practice on this critical care unit and the calculated indices do not currently influence patient management. Consequently, data acquired for the purpose of this paper did not require local ethical committee approval.
这种 MAP/ICP 监测是该重症医学科的标准临床实践,计算的指数目前不影响病人的管理。因此,为本文的目的而获得的数据不需要当地伦理委员会的批准。
Artifacts were identified and excluded from analysis after data collection was completed. Most artifacts were the result of disconnection of the patient from the monitoring system (e.g., for transport to the radiology department or the operating theater) or because of an inadequate pressure signal from the arterial catheter. A standardized computer algorithm was used for artifact recognition. It identified negative values for all pressures as they typically arise when patients are disconnected, rejected values for MAP and ICP if the amplitude of the traces was inadequate, and values for MAP and heart rate outside the physiologic range. When a measurement of one of the parameters was interpreted as an artifact at a certain time point, the values for all parameters at that time point were rejected. After removal of such time periods, the data plots were checked for missed artifacts, but no further data were excluded from analysis.
在数据收集完成后,识别出伪迹并从分析中排除。大多数假象是由于病人与监测系统断开连接(例如,运送到放射科或手术室)或由于动脉导管的压力信号不足造成的。一个标准化的计算机算法被用于识别伪影。它识别出所有压力的负值,因为它们通常是在病人断开连接时出现的,如果描记的振幅不足,则舍弃 MAP 和 ICP 的值,MAP 和心率超出生理范围的值也舍弃。当某一参数的测量被解释为某一时间点的伪影时,该时间点的所有参数值都被拒绝。剔除此类时间段后,检查数据图是否有遗漏的伪影,但不再有数据被排除出分析。
Outcome was assessed using the Glasgow Outcome Scale (GOS) ([12]) 6 months after discharge from the critical care unit. Patients were contacted and either evaluated at an appointment or by telephone using a questionnaire for a standardized interview ([13]). If necessary, a caregiver was interviewed instead.
从重症医学科出院后 6 个月,使用格拉斯哥结果量表(GOS)([12])评估预后。与患者联系,在预约时或通过电话使用标准化访谈的调查表([13])对患者进行评估。如果有必要的话,也会对其护理人员进行访谈。
数据分析
Values of measured variables from each patient were averaged over the whole monitoring period, so every patient was represented by one set of data containing MAP, ICP, CPP, and PRx. Correlations between these parameters, admission GCS, and GOS were calculated using Spearman's rank test. To test the hypothesis of a time-dependent impact of disturbed cerebrovascular pressure reactivity, the percentage of time each patient spent at PRx >0.2 was calculated. This value has been determined previously to form a threshold for a significant disturbance of pressure reactivity ([9, 10]). For the determination of CPPOPT in individual patients, CPP values were divided into groups of 5 mm Hg (e.g., 70-75 mm Hg) and PRx was averaged within these groups. Groups were excluded from analysis if they contained <2.5% of the patient's data sets. The value for CPPOPT was only accepted if the graph showed a distinct minimum value for mean PRx, i.e., mean values for PRx in both adjacent CPP groups were higher (for examples, see [Figs. 2 and 3]).
每位患者的测量变量值在整个监测期间取平均值,因此每位患者都由一组数据代表,其中包括 MAP、ICP、CPP 和 PRx。这些参数、入院时的 GCS 和 GOS 之间的相关性用 Spearman 排名检验来计算。为了检验脑血管压力反应性紊乱的时间依赖性影响的假设,计算了每个病人在 PRx>0.2 时的时间百分比。这个数值以前已经被确定为压力反应性明显紊乱的阈值([9, 10])。为了确定单个病人的 CPPOPT,CPP 值被分为 5mmHg 的组(如 70-75mmHg),PRx 在这些组内取平均值。如果组中包含 < 2.5% 的病人数据集,则排除在分析之外。CPPOPT 的值只有在图形显示平均 PRx 的明显最小值时才被接受,即相邻的两个 CPP 组的 PRx 的平均值都较高(例子见 [图 2 和 3])。
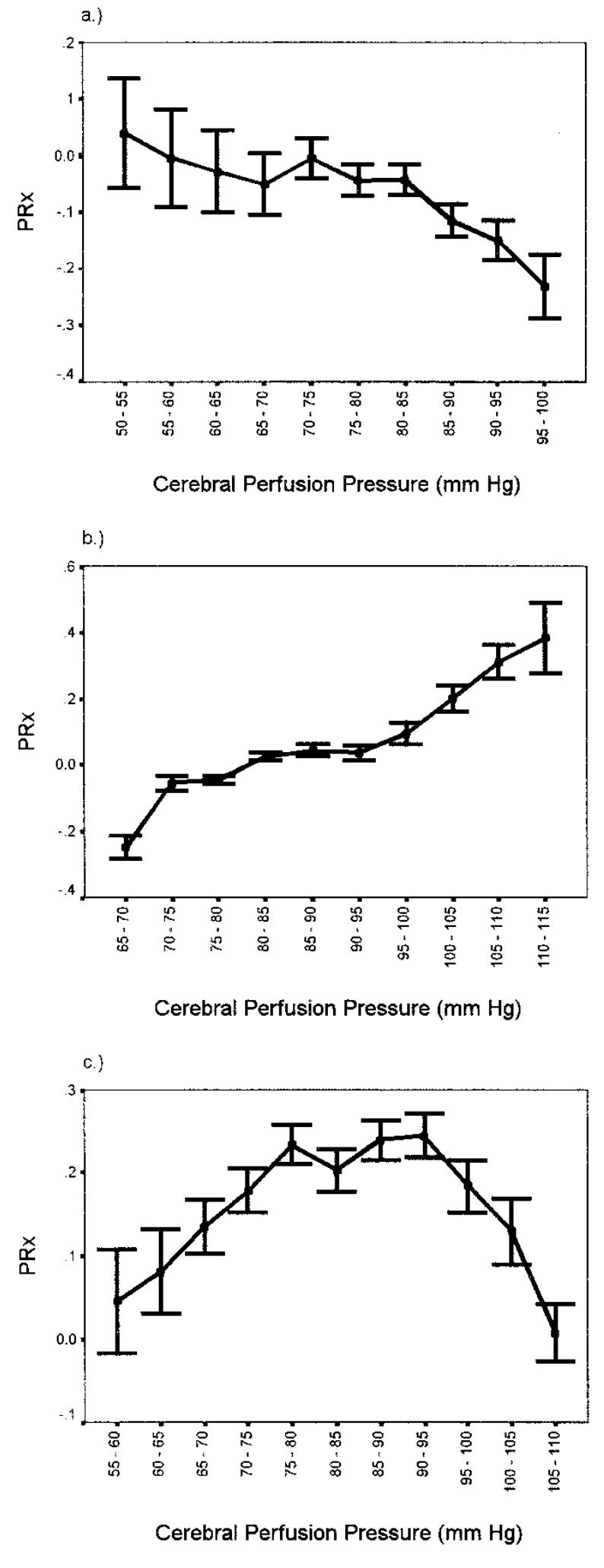
Figure 3. Examples of pressure reactivity index (PRx) vs. cerebral perfusion pressure (CPP) plots where determination of optimal cerebral perfusion pressure (CPPOPT) is not possible. Error bars represent 95% confidence intervals.
图 3. 压力反应性指数(PRx)与脑灌注压(CPP)不可能确定最佳脑灌注压(CPPOPT)的图例。误差条代表 95% 的置信区间。
In individual patients, the difference (in mm Hg) between CPPOPT and mean CPP for the whole monitoring period was calculated (CPP = CPP - CPPOPT). As CPPOPT can be located above or below the mean CPP, we analyzed the absolute difference |CPP - CPPOPT| as well as the differences for the groups with positive or negative values for CPP. Correlation to GOS was calculated using Spearman's rank test. For further analysis, outcome was dichotomized into good outcome (good recovery, moderate disability) and poor outcome (severe disability, persistent vegetative state, and dead). Groups were compared using the nonparametric Kruskal-Wallis test because the values in the majority of groups were not normally distributed.
在个别患者中,计算 CPPOPT 与整个监测期的平均 CPP 之间的差异(mm Hg)(CPP = CPP - CPPOPT)。由于 CPPOPT 可以位于平均 CPP 之上或之下,我们分析了绝对差异 | CPP-CPPOPT | 以及 CPP 为正值或负值的组的差异。与 GOS 的相关性是用 Spearman's rank test 计算的。为了进一步分析,结果被分为好的结果(恢复良好,中度残疾)和差的结果(严重残疾,持续植物状态,和死亡)。由于大多数组的数值不是正态分布,所以用非参数 Kruskal-Wallis 检验来比较各组。
结果
The total monitoring time amounted to 13,633 hrs (568 days) and 817,970 data sets containing MAP, ICP, CPP, and PRx were recorded. After artifact extraction, 727,651 data sets remained (89%). In individual patients, a mean of 11% of data were rejected (range 0.5% to 94%) The mean recording time per patient after artifact removal was 118 hrs (range 8-358 hrs). On average, 55 data sets per hour were available for further analysis (range 4-60).
总的监测时间为 13,633 小时(568 天),记录了 817,970 组数据,包括 MAP、ICP、CPP 和 PRx。在剔除伪像后,剩下 727,651 个数据集(89%)。在个别病人中,平均有 11% 的数据被拒绝(范围为 0.5% 至 94%)。在去除伪影后,每个病人的平均记录时间为 118 小时(范围为 8-358 小时)。平均每小时有 55 组数据可供进一步分析(范围 4-60)。
Spearman rank correlation coefficients and p values between the averaged values of MAP, ICP, CPP, PRx, admission GCS, and GOS are presented in [Table 2].
MAP、ICP、CPP、PRx、入院 GCS 和 GOS 的平均值之间的 Spearman 等级相关系数和 P 值见 [表 2]。
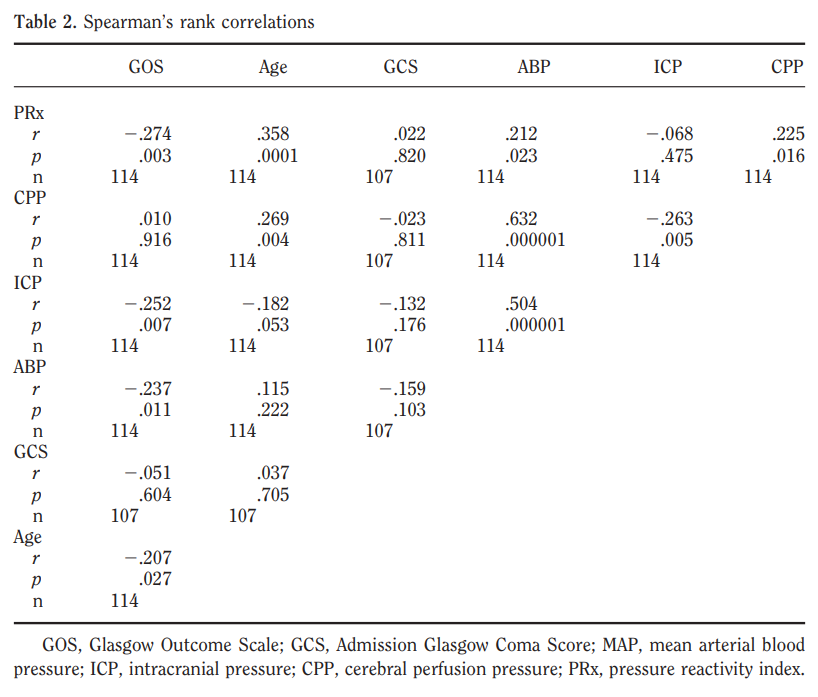
Table 2. Spearman's rank correlations
GOS, Glasgow Outcome Scale; GCS, Admission Glasgow Coma Score; MAP, mean arterial blood pressure; ICP, intracranial pressure; CPP, cerebral perfusion pressure; PRx, pressure reactivity index.
表 2. 斯皮尔曼等级相关性
GOS, 格拉斯哥预后量表;GCS, 入院格拉斯哥昏迷评分;MAP, 平均动脉压;ICP, 颅内压;CPP, 脑灌注压;PRx, 压力反应性指数.
The correlation between PRx and outcome was significant (r = -.27, p < .005) indicating that a higher value of PRx (cerebrovascular pressure reactivity is disturbed) is associated with a less favorable outcome. The impact of inadequate cerebrovascular reactivity was time dependent: The percentage of monitoring time each patient's PRx was >0.2 correlated significantly to outcome (r = -.28, p < .005). In this series of patients there was no significant relationship between PRx and CT findings or CT findings and outcome.
PRx 和预后之间的相关性很明显(r = -.27,p <.005),表明 PRx 的值越高(脑血管压力反应性受到干扰)与较差的结果有关。脑血管反应性不足的影响与时间有关。每个病人的 PRx>0.2 的监测时间的百分比与预后明显相关(r = -.28,p < .005)。在这个系列的病人中,PRx 和 CT 结果或 CT 结果和结果之间没有明显的关系。
PRx reacted dynamically to changes in CPP with breakpoints for a decline in cerebrovascular pressure reactivity at approximately 60 and 85 mm Hg when data from all patients was pooled ([Fig. 4]).
当汇集所有病人的数据时,PRx 对 CPP 的变化有动态反应,脑血管压力反应性下降的折点大约在 60 和 85mmHg([图 4])。
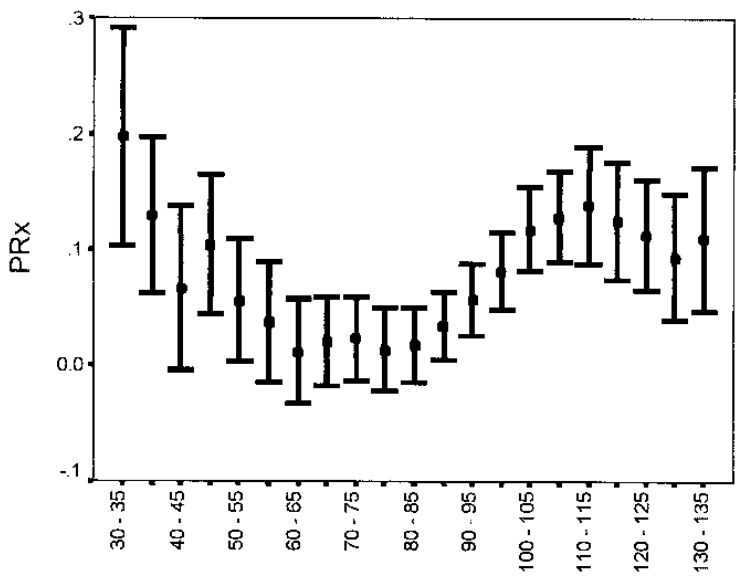
Figure 4. Pressure reactivity index (PRx) vs. cerebral perfusion pressure for all patients (n = 114). Below 60 and above 85 mm Hg cerebrovascular pressure reactivity deteriorates. Error bars represent 95% confidence intervals.
图 4. 所有患者(n = 114)的压力反应性指数(PRx)与脑灌注压的关系。低于 60 和高于 85 毫米汞柱的脑血管压力反应性会恶化。误差条代表 95% 的置信区间。
Determination of an individual CPPOPT was possible in 68 patients (60%). In 38 patients, mean CPP was below CPPOPT and in 30 patients, mean CPP was above CPPOPT. [Figure 5] shows the number of patients in each category of GOS in whom CPPOPT could not be determined and the number of patients whose CPPOPT was above or below mean CPP.
68 名患者(60%)可以确定个人 CPPOPT。38 名患者的平均 CPP 低于 CPPOPT,30 名患者的平均 CPP 高于 CPPOPT。[图 5] 显示了每一类 GOS 中无法确定 CPPOPT 的患者人数以及 CPPOPT 高于或低于平均 CPP 的患者人数。
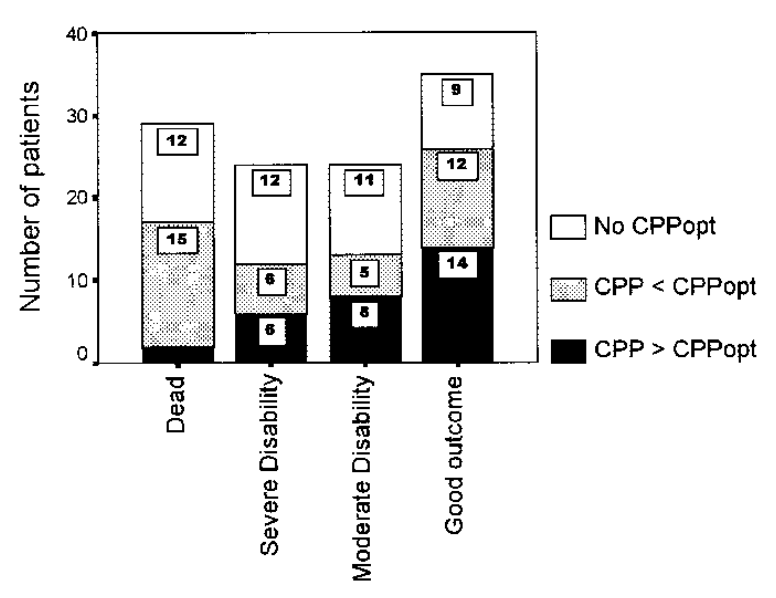
Figure 5. Distribution of patients into the categories of the Glasgow Outcome Score and number of patients with cerebral perfusion pressure (CPP) above, below, or without an optimal cerebral perfusion pressure (CPPOPT).
图 5. 患者在格拉斯哥上报评分中的分布,以及脑灌注压(CPP)高于、低于或没有最佳脑灌注压(CPPOPT)的患者数量。
The proportion of patients in whom no CPPOPT was detected did not differ significantly between categories of GOS. CPPOPT for patients with a poor outcome was significantly higher than CPPOPT for patients with a good outcome (p < .005). The correlation of ||CPP - CPPOPT|| to GOS was highly significant (r = -.51, p < .00001), demonstrating that the more CPP was different from CPPOPT the greater was the likelihood of an unfavorable outcome. The correlation between CPP and GOS was significant for patients with CPP < 0 (r = .53, p < .001) and patients with CPP > 0 (r = -.40, p < .05) showing that both a CPP that is too low and a CPP that is too high may have a negative impact on outcome. When patients are grouped into good and poor outcomes, CPP was significantly larger in patients with poor outcome compared with patients with good outcome irrespective of CPPOPT being above or below CPP ([Fig. 6]).
没有检测到 CPPOPT 的患者比例在不同类别的 GOS 之间没有显著差异。预后差的病人的 CPPOPT 明显高于预后好的病人的 CPPOPT(P < .005)。||CPP-CPP|| 与 GOS 的相关性非常显著(r = -.51,p < .00001),表明 CPP 与 CPPOPT 的差异越大,出现预后不佳的可能性就越大。 CPP 和 GOS 之间的相关性对于 CPP<0(r = .53,p < .001)和 CPP>0(r = -.40,p < .05)的患者是显著的,表明 CPP 太低和 CPP 太高都可能对结果产生负面影响。当患者按预后好坏分组时,无论 CPPOPT 高于或低于 CPP,预后差的患者与好的患者相比, CPP 都明显较大([图 6])。
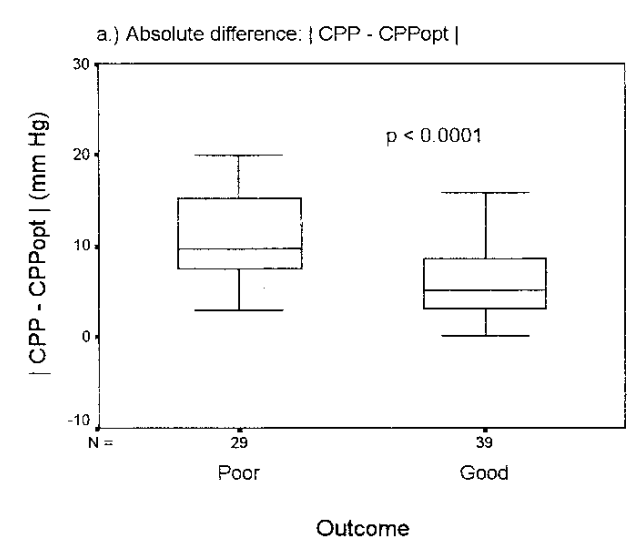
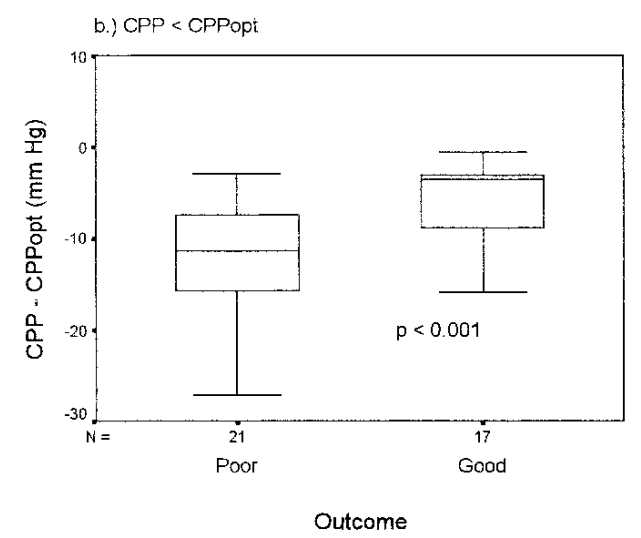
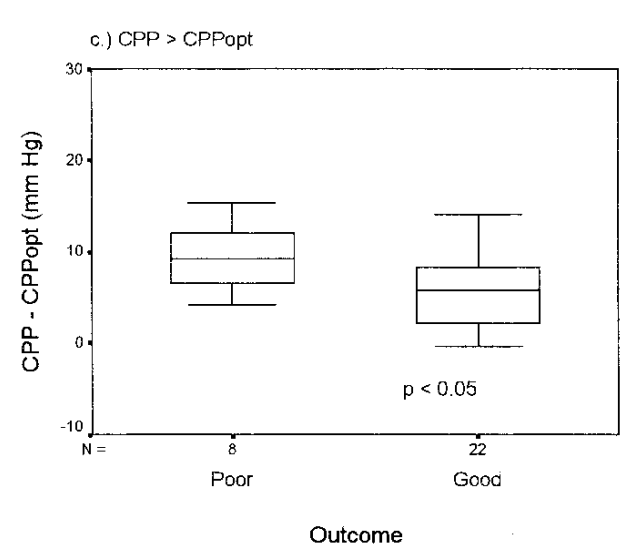
Figure 6. Box and whisker plots of dichotomized outcome vs. cerebral perfusion pressure (CPP) minus optimal cerebral perfusion pressure (CPPOPT) for (a) absolute difference; (b) CPPOPT > CPP; and (c) CPPOPT < CPP. Lines within boxes denote median. p Values were calculated using the Kruskal-Wallis test.
图 6. 二分法预后与脑灌注压(CPP)减去最佳脑灌注压(CPPOPT)的框须图
(a) 绝对差值;(b)CPPOPT>CPP;以及 (c) CPPOPT<CPP。
方框内的线表示中位数。 p 值用 Kruskal-Wallis 检验计算。
讨论
Using PRx to monitor cerebrovascular pressure reactivity, we have been able to retrospectively define CPPOPT in almost two thirds of patients in this large group of head-injured patients. Because of the significant correlation between outcome and CPP, we propose use of CPPOPT as a target for managing CPP after head injury.
使用 PRx 监测脑血管压力反应性,我们已经能够回顾性地确定这个大型脑外伤患者群体中几乎三分之二的患者的 CPPOPT。由于结果与 CPP 之间存在明显的相关性,我们建议将 CPPOPT 作为脑外伤后管理 CPP 的目标。
### 方法学问题
Methodologic Issues.
In 40% of our patients we were not able to identify CPPOPT. The most frequent reason (22 patients) that prevented us from identifying CPPOPT was the situation shown in [Figure 3, a and b]. We interpret this pattern as reflecting a CPPOPT that lies outside the range of CPP studied. It is reasonable to expect that, if CPP is targeted toward a more favorable range of PRx, it will be possible to define CPPOPT within the next few hours of monitoring. Another possible explanation for failing to define CPPOPT is an insufficient number of data sets either because the recording time was too short (four patients) or because of a high rate of artifacts. CPPOPT can only be determined after the patient has been monitored for several hours. The smallest number of data sets that allowed for determination of CPPOPT was 922 corresponding to a monitoring time of 19 hrs. Generally, 24 hrs were sufficient to collect an adequate number of data sets with which to calculate CPPOPT. Artifacts were not a major problem, mainly because patients were paralyzed. As soon as paralysis and sedation were stopped and weaning from artificial ventilation was started, the artifact rate increased. However, by this time ICP is generally normal and CPP stable. Another reason for CPPOPT not being demonstrable were varying values for CPPOPT over time that were missed because we averaged data over the whole monitoring period. This has possibly been the case in a single patient in this series and would be avoided if CPPOPT were calculated as a moving average over the last 24 hrs. Another very important explanation for not being able to define CPPOPT could be that CPPOPT does not exist when cerebrovascular pressure reactivity is severely compromised for other reasons than an inadequate CPP. This was possibly the case in the patient shown in [Figure 3c] (PRx > 0.2 for CPP varying from 75 to 95 mm Hg). Severe disturbance of cerebrovascular pressure reactivity would be expected most often in the most severely injured patients. Fittingly, this pattern was only observed in four patients with a poor outcome. Finally, it is possible that the type of vasopressor management or the use of mannitol influences the relationship between PRx and CPP, but our data does not allow us to explore this and it is the subject of further prospective study.
在我们的病人中,有 40% 的病人我们无法识别 CPPOPT。妨碍识别 CPPOPT 的最常见原因(22 名患者)是 [图 3,a 和 b] 中所示的情况。这种模式意味着 CPPOPT 位于研究中测量 CPP 的范围之外。我们有理由期待,如果 CPP 向着更有利的 PRx 范围的方向变化,就有可能在接下来的几个小时的监测中确定 CPPOPT。未能确定 CPPOPT 的另一个可能的解释是数据集的数量不足,要么是因为记录时间太短(4 个病人),要么是因为伪影率高。CPPOPT 只有在对病人进行数小时的监测后才能确定。能够确定 CPPOPT 的最小数据集是 922 个,对应的监测时间为 19 小时。一般来说,24 小时足以收集足够数量的数据集,以计算 CPPOPT。伪影不是一个主要的问题,主要是因为病人是肌松的。一旦停止肌松和镇静,开始撤掉人工呼吸,伪影率就会增加。然而,这时 ICP 一般是正常的,CPP 也是稳定的。CPPOPT 不明显的另一个原因是 CPPOPT 随时间变化的数值,因为我们对整个监测期的数据进行了平均,所以会漏掉。本系列病例某个病人可能出现这种情况,如果 24 小时的时间内将 CPPOPT 作为移动平均值来计算,就可以避免这种情况。无法确定 CPPOPT 的另一个非常重要的解释是,当脑血管压力反应性因 CPP 不足的其他原因而严重受损时,CPPOPT 并不存在。图 3c 中的病人可能就是这种情况(CPP 在 75 至 95mmHg 之间时,PRx>0.2)。脑血管压力反应性的严重紊乱预计最常发生在受伤最严重的病人身上。所幸,这种模式只在四名结果不佳的病人身上观察到。最后,血管收缩剂应用的类型或甘露醇的使用有可能影响 PRx 和 CPP 之间的关系,但我们的数据不允许我们对此进行探讨,这是进一步前瞻性研究的主题。
最佳 CPP
Optimal CPP.
The need to define what is the target CPP for an individual patient after head injury has been stressed by several authors ([14, 15]). Patterns of injury are highly variable and it is unlikely that one threshold will be optimal for all patients. As a result, recommendations for target values of CPP after head injury range from 60 mm Hg and lower ([16]) to 85 mm Hg and higher ([14]). Interestingly, this range of CPP is almost identical to the range of CPP that lies between the upper and lower breakpoints of CPP versus PRx shown in [Figure 4]. For individual patients, however, this range is too large, as is reflected by the relatively small difference of CPP between patients with favorable and unfavorable outcomes (mean CPP 6 and 11 mm Hg, respectively, [Fig. 6a]). The fact that the individual range of suitable CPP is much smaller than the range found for the whole group of patients also explains the lack of an overall correlation between outcome and CPP in our patients. This result is in agreement with another recent large study of 427 patients who did not find a correlation between CPP and outcome after head injury where CPP was >60 mm Hg ([17]).
有几位作者强调,有必要为脑外伤后的病人个体确定目标 CPP 是什么([14, 15])。损伤模式差异极大,一个阈值不可能对所有病人都是最佳的。因此,对脑外伤后 CPP 目标值的建议范围从低至 60 mm Hg 及以下([16])到高达 85 mm Hg 及以上([14])。有趣的是,这个 CPP 的范围几乎与 [图 4] 所示的 CPP 与 PRx 的上下限之间的 CPP 范围相同。然而,对于个别病人来说,这个范围太大,这可以从预后好与不好的病人之间相对较小的 CPP 差值反映出来(平均 CPP 6 和 11 mm Hg,[图 6a])。合适的 CPP 的个体范围远远小于为整组患者确定的范围,这也解释了在我们的患者中,预后和 CPP 之间缺乏整体相关性。这一结果与最近另一项针对 427 名患者的大型研究相一致,该研究没有发现 CPP 与脑外伤后的预后之间存在相关性,其 CPP>60mmHg([17])。
以自动调节为导向的治疗
Autoregulation-Oriented Therapy.
Several authors have proposed that the state of cerebrovascular autoregulation should be integrated into management plans ([15, 18-20]). The problem with such an approach is how to assess autoregulation continuously. CPPOPT-based management is one possible autoregulation-oriented strategy, despite the fact that PRx does not precisely represent autoregulation. The correlation between outcome and PRx, as well as the time-dependent impact of PRx on outcome are strong indicators that cerebrovascular pressure reactivity is a suitable parameter on which an autoregulation-oriented treatment strategy can be based. There is an additional aspect to the use of CPPOPT: In contrast to a simple threshold above which CPP is held, CPPOPT-guided therapy can help to avoid inappropriately high CPP. It is not surprising that a CPP greater than CPPOPT shows a correlation to outcome, as does a CPP below CPPOPT. Excessively high CPP can lead to disruption of the blood-brain barrier ([21]), development of vasogenic edema ([22]), and may predispose to cardiac dysfunction ([23]). In view of our data, we may possibly be overtreating some of our patients (almost a third in this series) by keeping CPP above CPPOPT. To use a less aggressive treatment strategy would probably be beneficial in these patients. The determination of CPPOPT as a guide for an upper limit for CPP may also be useful in other patient groups, for example, patients after subarachnoid hemorrhage who are treated with induced hypertension.
一些作者提出,应将脑血管自动调节状态纳入管理计划([15, 18-20])。这种方法的问题是如何连续评估自动调节。基于 CPPOPT 的管理是一种可能的以自动调节为导向的策略,尽管 PRx 并不能精确代表自动调节。疗效与 PRx 之间的相关性以及 PRx 对疗效的时间影响有力地表明,脑血管压力反应性是一个合适的参数,以自动调节为导向的治疗策略可以以此为基础。使用 CPPOPT 还有一个方面。与一个简单的阈值相比,CPPOPT 指导的治疗可以帮助避免不适当的高 CPP。大于 CPPOPT 的 CPP 和低于 CPPOPT 的 CPP 一样,显示出与预后的相关性,这并不奇怪。过高的 CPP 可导致血脑屏障的破坏([21]),发展为血管性水肿([22]),并可能导致心脏功能障碍([23])。从我们的数据来看,我们可能将 CPP 保持在 CPPOPT 以上,从而一些患者受到了过度治疗(本系列中几乎占三分之一)。对这些病人采用不太积极的治疗策略可能会有好处。确定 CPPOPT 作为 CPP 上限的指导也可能对其他患者群体有用,例如蛛网膜下腔出血后实施诱导性高血压治疗的患者。
预后
Outcome.
In this study, there was no correlation between outcome and admission GCS, which is generally accepted as a good predictor of outcome after head injury ([24]). We suspect that this is a consequence of improved prehospital care with a greater number of patients being intubated at the scene of the accident. This will often lead to a spuriously low GCS at admission. The same problem occurs when patients are transferred from other hospitals, which was the case in about 25% of our patients. Additional indicators of severity of trauma such as grading according to CT scans are clearly necessary. Further studies are needed to characterize the relationship between various patterns of injury as seen on CT and autoregulation. The fact that the patients with unfavorable outcome had significantly higher CPPOPT values suggests that the absolute value of CPPOPT and the corresponding value of PRx may possibly be indicators of the severity of the head injury.
在这项研究中,结果与入院时的 GCS 没有关联,而 GCS 被公认为是预测脑外伤后上报的良好指标([24])。我们怀疑这是院前救治改善的结果,更多的病人在事故现场就插管。这往往会导致入院时 GCS 假性偏低。当病人从其他医院转来时也会出现同样的问题,我们的病人中约有 25% 是这种情况。显然,有必要制定额外的创伤严重性指标,如根据 CT 扫描进行分级。需要进一步的研究来确定 CT 上看到的各种损伤模式与自动调节之间的关系。预后不佳患者的 CPPOPT 值明显较高,这表明 CPPOPT 的绝对值和 PRx 的相应值可能是头部损伤严重程度的指标。
推荐的治疗方案
Proposed Management Protocol.
This study reports a retrospective observation and further prospective studies are needed to support our hypothesis that managing patients at about CPPOPT will be beneficial. It is important to note that such an approach will be demanding for the physicians and nurses involved as the range in which CPP should be kept is quite narrow: CPPOPT +/- 5 mm Hg (see [Fig. 6]). One possible criticism of our approach is that approximately a 24-hr interval is needed to define CPPOPT. However, it will probably be possible to reduce this time by initially choosing a CPP that seems likely to be near CPPOPT and monitor PRx over 2 hrs, then change CPP upwards by 10 mm Hg and observe the trend in PRx. If mean PRx drops over the next 2 hrs, CPP can be raised another 10 mm Hg; if PRx rises, CPP can be reduced 10 mm Hg beyond the initial CPP and again the trend in PRx is observed over 2 hrs. This procedure can be repeated until a minimum of PRx can be identified. Using this approach it should be possible to define CPPOPT within 6-10 hrs. It is important to note that such an approach depends on a stable value for CPPOPT over time and we are our currently adjusting our method to allow measuring short time variability of CPPOPT. The proposed algorithm ([Fig. 7]) will be tested in a prospective study.
本研究报告了一个回顾性的观察,需要进一步的前瞻性研究来支持我们的假设,即在 CPPOPT 附近管理病人会获益。值得注意的是,这种方法对医生和护士的要求很高,因为 CPP 应保持在相当窄的范围内。CPPOPT +/- 5 mm Hg(见 [图 6])。该方法可能被批评的一点是,需要大约 24 小时的间隔来确定 CPPOPT。然而,有可能减少这个时间,最初选择一个可能接近 CPPOPT 的 CPP,监测 PRx 超过 2 小时,然后将 CPP 向上改变 10mmHg,观察 PRx 的趋势。如果平均 PRx 在接下来的 2 小时内下降,CPP 可以再提高 10 毫米汞柱;如果 PRx 上升,CPP 可以降低 10 毫米汞柱,超过最初的 CPP,再次观察 2 小时内 PRx 的趋势。这个过程可以重复进行,直到可以确定 PRx 的最低值。使用这种方法,应该可以在 6-10 小时内确定 CPPOPT。值得注意的是,这种方法取决于 CPPOPT 在一段时间内的稳定值,我们目前正在调整我们的方法以允许测量 CPPOPT 的短时间变化。建议的算法([图 7])将在一项前瞻性研究中进行测试。
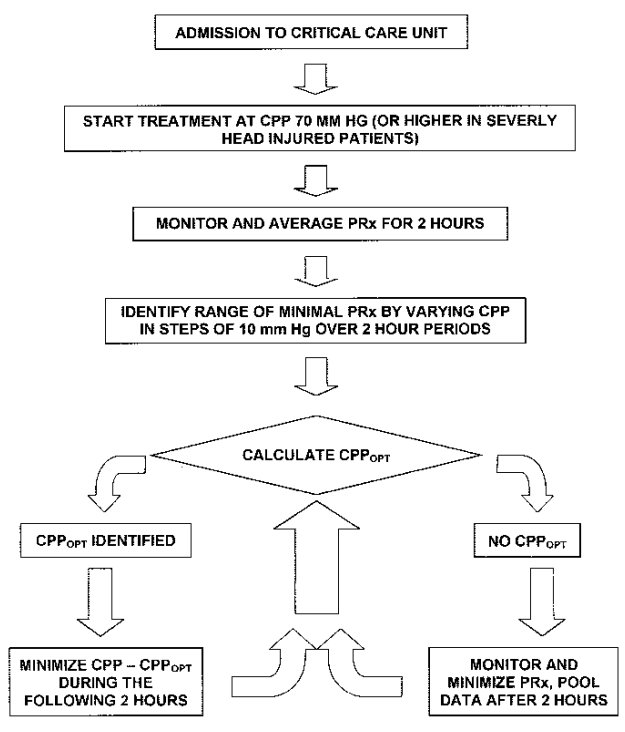
Figure 7. Proposed algorithm for an autoregulation-oriented, pressure reactivity index (PRx)-guided approach to cerebral perfusion pressure (CPP) management after head injury that will hypothetically allow optimization of individual CPP. CPPOPT, optimal cerebral perfusion pressure.
图 7. 自动调节导向、压力反应指数(PRx)指导的脑外伤后脑灌注压(CPP)管理方法的推荐流程,假设个体 CPP 能进一步优化。CPPOPT,最佳脑灌注压。
The software we currently use ([11]) needs to be adapted so that CPPOPT can be determined as a moving average at the bedside. The displaying of mean values of PRx in addition to CPPOPT will be helpful in the management of those patients where no CPPOPT can be identified and during the first hours before CPPOPT can be calculated.
我们目前使用的软件([11])尚需调整,以便可以在床边以移动平均的方式确定 CPPOPT。除了 CPPOPT 之外,显示 PRx 的平均值将有助于管理那些无法确定 CPPOPT 的患者,以及 CPPOPT 结果出来前的最初几个小时内的患者。
结论
Continuous longtime monitoring of PRx in head-injured patients enabled the determination of a CPP at which cerebrovascular pressure reactivity reached its optimal value in an individual patient in almost two thirds of the investigated patients. We propose that CPPOPT should be assessed as an individual target value in future trials of CPP oriented therapy after head injury. This concept is supported by the correlation between CPP and outcome. Prospective studies are required to evaluate the benefit of this autoregulation-oriented approach.
对脑外伤患者的 PRx 进行连续的长时间监测,能够确定一个 CPP,在这个 CPP 下,几乎三分之二的被调查患者的脑血管压力反应性达到最佳值。我们建议,在未来的脑外伤后以 CPP 为导向的治疗试验中,应将 CPPOPT 作为个体目标值进行评估。CPP 和预后之间的相关性支持这一概念。尚需进行前瞻性研究来评估这种自动调节导向方案的益处。
REFERENCES
1. Paulson OB, Strandgaard S, Edvinsson L: Cerebral autoregulation. Cerebrovasc Brain Metab Rev 1990; 2: 161-192.
大脑自动调节。
2. MacKenzie ET, Farrar JK, Fitch W, et al: Effects of hemorrhagic hypotension on the cerebral circulation. I. Cerebral blood flow and pial arteriolar caliber. Stroke 1979; 10: 711-718.
出血性低血压对大脑循环的影响。I. 脑血流和小动脉血管口径。
3. Rosner MJ, Becker DP: Origin and evolution of plateau waves. Experimental observations and a theoretical model. J Neurosurg 1984; 60: 312-324.
高原波的起源和演变:实验观察和一个理论模型。
4. Barzo P, Bari F, Doczi T, et al: Significance of the rate of systemic change in blood pressure on the short-term autoregulatory response in normotensive and spontaneously hypertensive rats. Neurosurgery 1993; 32: 611-618
4. Barzo P, Bari F, Doczi T, et al: 血压的系统变化率对正常血压和自发性高血压大鼠的短期自动调节反应的意义。
5. Maset AL, Marmarou A, Ward JD, et al: Pressure-volume index in head injury. J Neurosurg 1987; 67: 832-840.
头部损伤的压力 - 容积指数。
6. Muizelaar JP, Ward JD, Marmarou A, et al: Cerebral blood flow and metabolism in severely head-injured children. Part 2: Autoregulation. J Neurosurg 1989; 71: 72-76.
严重脑外伤儿童的脑血流和代谢。第二部分:自动调节。
7. Lang EW, Chesnut RM: Intracranial pressure and cerebral perfusion pressure in severe head injury. New Horiz 1995; 3: 400-409.
严重头部损伤的颅内压和脑灌注压。
8. Steinmeier R, Bauhuf C, Hubner U, et al: Slow rhythmic oscillations of blood pressure, intracranial pressure, microcirculation, and cerebral oxygenation. Dynamic interrelation and time course in humans. Stroke 1996; 27: 2236-2243.
血压、颅内压、微循环和脑氧饱和度的缓慢节律性震荡。人类的动态相互关系和时间过程。
9. Czosnyka M, Smielewski P, Kirkpatrick P, et al: Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery 1997; 41: 11-17.
连续评估脑外伤的脑血管运动反应性。
10. Czosnyka M, Smielewski P, Kirkpatrick P, et al: Continuous monitoring of cerebrovascular pressure-reactivity in head injury. Acta Neurochir Suppl 1998; 71: 74-77.
连续监测脑外伤的脑血管压力反应性。
11. Czosnyka M, Whitehouse H, Smielewski P, et al: Computer supported multimodal bed-side monitoring for neuro intensive care. Int J Clin Monit Comput 1994; 11: 223-232.
计算机支持的神经重症监护的床边多模式监测。
12. Jennett B, Bond M: Assessment of outcome after severe brain damage. Lancet 1975; 1: 480-484.
严重脑损伤后的结果评估。
13. Wilson JT, Pettigrew LE, Teasdale GM: Structured interviews for the Glasgow Outcome Scale and the extended Glasgow Outcome Scale: Guidelines for their use. J Neurotrauma 1998; 15: 573-585.
格拉斯哥结果量表和扩展格拉斯哥结果量表的结构化访谈。他们的使用指南。
14. Rosner MJ, Rosner SD, Johnson AH: Cerebral perfusion pressure: Management protocol and clinical results. J Neurosurg 1995; 83: 949-962
14. Rosner MJ, Rosner SD, Johnson AH: 大脑灌注压:管理方案和临床结果。J Neurosurg 1995; 83: 949-962
15. Lang EW, Chesnut RM: A bedside method for investigating the integrity and critical thresholds of cerebral pressure autoregulation in severe traumatic brain injury patients. Br J Neurosurg 2000; 14: 117-126.
调查严重脑外伤患者脑压自动调节的完整性和关键阈值的床边方法。
16. Eker C, Asgeirsson B, Grande PO, et al: Improved outcome after severe head injury with a new therapy based on principles for brain volume regulation and preserved microcirculation. Crit Care Med 1998; 26: 1881-1886.
基于脑容量调节和保留微循环原则的新疗法,改善了严重脑外伤后的结果。
17. Juul N, Morris GF, Marshall SB, et al: Intracranial hypertension and cerebral perfusion pressure: influence on neurological deterioration and outcome in severe head injury. The Executive Committee of the International Selfotel Trial. J Neurosurg 2000; 92: 1-6
17. Juul N, Morris GF, Marshall SB, et al: 颅内高压和脑灌注压:对严重脑外伤的神经系统恶化和结果的影响。国际 Selfotel 试验的执行委员会。J Neurosurg 2000; 92: 1-6
18. Chesnut RM: Medical management of severe head injury: present and future. New Horiz 1995; 3: 581-593
18. Chesnut RM: 严重头部伤害的医疗管理:现在和未来。New Horiz 1995; 3: 581-593
19. Sahuquillo J, Poca MA, Ausina A, et al: Arterio-jugular differences of oxygen (AVDO2) for bedside assessment of CO2-reactivity and autoregulation in the acute phase of severe head injury. Acta Neurochir 1996; 138: 435-444
19. Sahuquillo J, Poca MA, Ausina A, et al: 严重颅脑损伤急性期床边评估 CO2/reactivity 和自动调节的动脉 - 颈部氧气差异(AVDO2)。Acta Neurochir 1996; 138: 435-444
20. Mascia L, Andrews PJ, McKeating EG, et al: Cerebral blood flow and metabolism in severe brain injury: the role of pressure autoregulation during cerebral perfusionpressure management. Intensive Care Med 2000; 26: 202-205
20. Mascia L, Andrews PJ, McKeating EG, et al: 严重脑损伤的脑血流和新陈代谢:脑灌注压管理期间压力自动调节的作用。重症监护医学 2000; 26: 202-205
21. MacKenzie ET, Strandgaard S, Graham DI, et al: Effects of acutely induced hypertension in cats on pial arteriolar caliber, local cerebral blood flow, and the blood-brain barrier. Circ Res 1976; 39: 33-41.
急性诱导的猫的高血压对动脉血管口径、局部脑血流和血脑屏障的影响。
22. Durward QJ, Del Maestro RF, Amacher AL, et al: The influence of systemic arterial pressure and intracranial pressure on the development of cerebral vasogenic edema. J Neurosurg 1983; 59: 803-809.
全身动脉压和颅内压对脑血管性水肿发展的影响。
23. Kassell NF, Peerless SJ, Durward QJ, et al: Treatment of ischemic deficits from vasospasm with intravascular volume expansion and induced arterial hypertension. Neurosurgery 1982; 11: 337-343.
用血管内容量扩张和诱导动脉高血压治疗血管痉挛引起的缺血性障碍。
24. Cho DY, Wang YC: Comparison of the APACHE III, APACHE II and Glasgow Coma Scale in acute head injury for prediction of mortality and functional outcome. Intensive Care Med 1997; 23: 77-84.
急性颅脑损伤中 APACHE III、APACHE II 和 Glasgow 昏迷量表在预测死亡率和功能结局方面的比较。

 连续监测脑血管压力反应性可以确定创伤性脑损伤患者的最佳脑灌注压力
连续监测脑血管压力反应性可以确定创伤性脑损伤患者的最佳脑灌注压力