
 脑血流自动调节-血压对脑血流的影响
脑血流自动调节-血压对脑血流的影响
# 脑血流的自动调节:动脉血压对通过大脑皮层的血流的影响
Autoregulation of cerebral blood flow: influence of the arterial blood pressure on the blood flow through the cerebral cortex
A. MURRAY HARPER
From the University of Glasgow, Wellcome Surgical Research Laboratory, Bearsden Road, Bearsden, Glasgow 来自格拉斯哥大学,惠康外科研究实验室,比尔斯登路,比尔斯登,格拉斯哥
Harper AM. Autoregulation of cerebral blood flow: influence of the arterial blood pressure on the blood flow through the cerebral cortex. J Neurol Neurosurg Psychiatry. 1966;29(5):398-403. doi:10.1136/jnnp.29.5.398
DeepL 翻译# 序言
Until fairly recently it was believed that cerebral blood flow followed more or less passively the mean arterial blood pressure, and the stability of the cerebral circulation under physiological conditions reflected only the relative constancy of the arterial pressure maintained by the homeostatic pressor reflex mechanism (Sokoloff, 1959). That there might also be an intrinsic regulation of cerebrovascular tone was suggested by Fog (1934, 1938) and by Forbes, Nason, and Wortman (1937). These workers observed that the blood vessels of the pia mater constricted in response to a rise in arterial blood pressure and dilated in response to a fall in pressure.
直到最近,人们还认为脑血流或多或少是被动地跟随平均动脉血压,生理条件下脑循环的稳定性只反映了由稳压反射机制维持的动脉压力的相对稳定性(Sokoloff, 1959)。Fog(1934 年,1938 年)和 Forbes、Nason 和 Wortman(1937 年)提出,脑血管张力也可能有内在的调节。这些研究人员观察到,当动脉血压升高时,脑膜的血管收缩,当压力下降时,血管扩张。
Although more recent studies in man (summarized by Lassen, 1959) seem to refute the idea of a passive pressure/flow relationship for the cerebral circulation, there is still conflict on the precise role of the arterial blood pressure in the control of the cerebral blood flow.
尽管最近对人的研究(由 Lassen 总结,1959 年)似乎反驳了脑循环的被动压力 / 流量关系的观点,但对动脉血压在控制脑血流中的确切作用仍然存在冲突。
The experiments reported in this paper were undertaken to measure the effect of gradual reduction of the mean arterial blood pressure on the blood flow through the cerebral cortex under normal respiratory conditions (that is a PaCO2 of 40 mm.Hg) and under conditions of hypercapnia (CO2 being added to the respiratory mixture).
本文报告的实验是为了测量在正常呼吸条件下(即 PaCO2 为 40mm.Hg)和高碳酸血症条件下(二氧化碳被添加到呼吸混合物中),逐渐降低平均动脉血压对通过大脑皮层的血流的影响。
# 方法
One hundred and seventeen measurements of blood flow through the cerebral cortex were made on 12 unselected mongrel dogs. The animals were anaesthetized with thiopentone. A cuffed endotracheal tube was inserted and connected to a Starling respiratory pump, through which a 4:1 mixture of N20 and oxygen was delivered in open circuit. Suxamethonium chloride was administered at intervals. Repeated small doses of thiopentone were given during the actual operation. A cannula was inserted into the femoral artery and connected to a damped mercury manometer for the measurement of the systemic blood pressure. This cannula was also used for the withdrawal of arterial blood samples.
对 12 只未经挑选的杂种狗进行了 117 次大脑皮层血流的测量。用硫喷酮对这些动物进行了麻醉。插入带袖带的气管导管并与斯塔林呼吸泵相连,通过该呼吸泵以开路方式输送 4:1 的 N20 和氧气混合物。每隔一段时间施用氯化苏胺。在实际操作过程中,反复给予小剂量的硫喷酮。将一根插管插入股动脉并与阻尼式水银压力计相连,以测量全身血压。这根插管也被用于抽取动脉血样。
The thyroid branch of the common carotid artery was cannulated centripetally, the distal end being tied. The temporal muscle was excised and a trephine hole made over the perietal bone. A cruciate incision was made in the dura and the exposed brain cortex was covered with a plastic membrane (Melinex) 6p in thickness. A thin lead shield was placed over the surrounding dura and bone, leaving exposed only the area of cortex covered by the membrane. An end window Geiger counter, mounted 1 mm. above the exposed cortex, was connected to a ratemeter and.a direct writing recorder. After the operation was completed, thiopentone administration was discontinued and the preparation remained undisturbed for one hour before the first measurements of blood flow were made. Plasma substitute (Dextran), saturated with 85 Krypton, was injected, rapidly at first and then more slowly, into the carotid artery over two to three minutes. The blood flow through the cerebral cortex was calculated from the half-life of the initial slope of a semi-logarithmic plot of the clearance curve using the formula of Lassen and Ingvar (1961), Ingvar and Lassen (1962). After each measurement of blood flow, blood samples were taken from the femoral artery for the measurement of PaCO, and pH on the micro-Astrup apparatus. Arterial oxyhaemoglobin saturation was measured at intervals on a Kipp haemoreflector. Pharyngeal temperatures were measured with a mercury thermometer.
颈总动脉的甲状腺分支被向中心插管,远端被绑住。切除颞部肌肉,并在顶骨上开一个挖孔。在硬脑膜上做一个十字形切口,用厚度为 6p 的塑料膜(Melinex)覆盖暴露的大脑皮层。在周围的硬脑膜和骨头上放置一个薄的铅罩,只留下被膜覆盖的皮质区域。在暴露的皮层上方 1 毫米处安装了一个内窗盖格计数器,并与测速仪和直写记录器相连。操作完成后,停止使用硫喷酮,在进行第一次血流测量前,准备工作保持不受干扰一小时。用 85 氪饱和的血浆替代品(Dextran)在两到三分钟内快速注入颈动脉,然后再缓慢注入。根据 Lassen 和 Ingvar (1961), Ingvar 和 Lassen (1962) 的公式,用清除曲线的半对数图的初始斜率的半衰期来计算通过大脑皮层的血流量。每次测量完血流量后,从股动脉取血样,在微型阿斯特鲁普仪器上测量 PaCO 和 pH。动脉氧合血红蛋白饱和度每隔一段时间用 Kipp 血液反射器测量。咽部温度是用水银温度计测量的。
The experiments were divided into two groups:
GROUP 1: BLOOD PRESSURE REDUCTION DURING NORMOCAPNIA The mean arterial blood pressure was gradually lowered in eight dogs by bleeding the animals into a reservoir flask. The PaCO2 was held between 30 and 40 mm.Hg by adjusting the respirator.
实验被分为两组。
第一组:正常抽血时的血压降低 通过将动物放血到一个贮液瓶中,逐渐降低 8 只狗的平均动脉血压。通过调整呼吸器使 PaCO2 保持在 30 和 40mm.Hg 之间。
GROUP 2: BLOOD PRESSURE REDUCTION DURING HYPERCAPNIA The PCO2 was raised to, and maintained at, 68-86 mm.Hg (mean values) by adding carbon dioxide to the anaesthetic mixture in four dogs. The arterial blood pressure was then gradually lowered by bleeding them into the reservoir flask.
第二组:在高压状态下降低血压 通过在四只狗的麻醉混合物中加入二氧化碳,将 PCO2 提高到并保持在 68-86mm.Hg(平均值)。然后通过向贮液瓶中放血来逐渐降低动脉血压。
# 结果
GROUP 1: BLOOD PRESSURE REDUCTION DURING NORMOCAPNIA The results are given in Table I and Figure 1. The mean initial blood pressure from the experiments in this group was 155 mm.Hg. (The PaCO2 was held within fairly narrow limits for each dog.) The mean PaCO2 was 35-3 mm.Hg and the average standard deviation of PaCO2 in in- dogs was 6.6%.
第 1 组:正常麻醉过程中的血压降低 结果见表 I 和图 1。本组实验的平均初始血压为 155mm.Hg。(平均 PaCO2 为 35-3 mm.Hg,狗的 PaCO2 的平均标准偏差为 6.6%。
From Fig. 1 it can be seen that the blood pressure could be lowered to approximately 90 mm.Hg without any marked change in blood flow. At lower blood pressures, however, blood flow declined with blood pressure.
从图 1 可以看出,血压可以降低到大约 90 毫米汞柱,而血流量没有任何明显的变化。然而,在较低的血压下,血流量随着血压的下降而下降。
Over a fairly wide range of blood pressure (from 90 to 180 mm.Hg) the blood flow remained relatively constant, despite a varying blood pressure. This phenomenon will hereafter be referred to as autodividual regulation .
在相当宽的血压范围内(从 90 到 180 毫米汞柱),尽管血压在变化,但血流量仍然相对稳定。这种现象将在下文中被称为个体调节。
GROUP 2: BLOOD PRESSURE REDUCTION DURING HYPERCAPNiA The results are given in Table II. A blanket graph of all the results in this group is shown on Figure 2.
第二组:高血压时的血压下降 结果见表二。该组所有结果的总图见图 2。
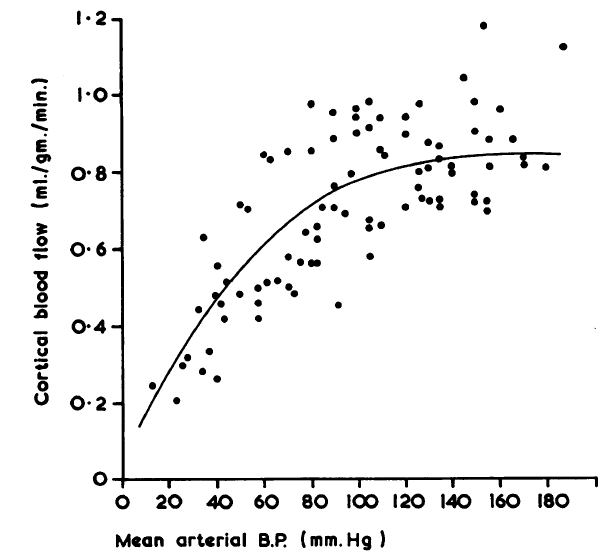
FIG. 1. Response ofcortical bloodflow to changes in mean arterial bloodpressure in normocapnic animals. Line is best polynomial fit.
图 1. 皮质血流对常压动物平均动脉血压变化的反应。线是最佳多项式拟合。
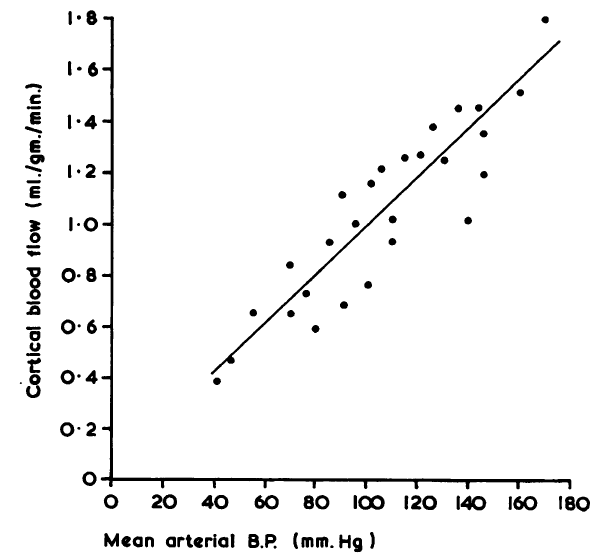
FIG. 2. Response to cortical bloodflow to changes in mean arterial blood pressure in hypercapnic animals. Line is calculated linear regression.
图 2. 皮质血流对高碳酸血症动物平均动脉血压变化的反应。线是计算出来的线性回归。
TABLE II HYPOTENSION AT HYPERCAPNIA
表二 高碳酸血症时的低血压
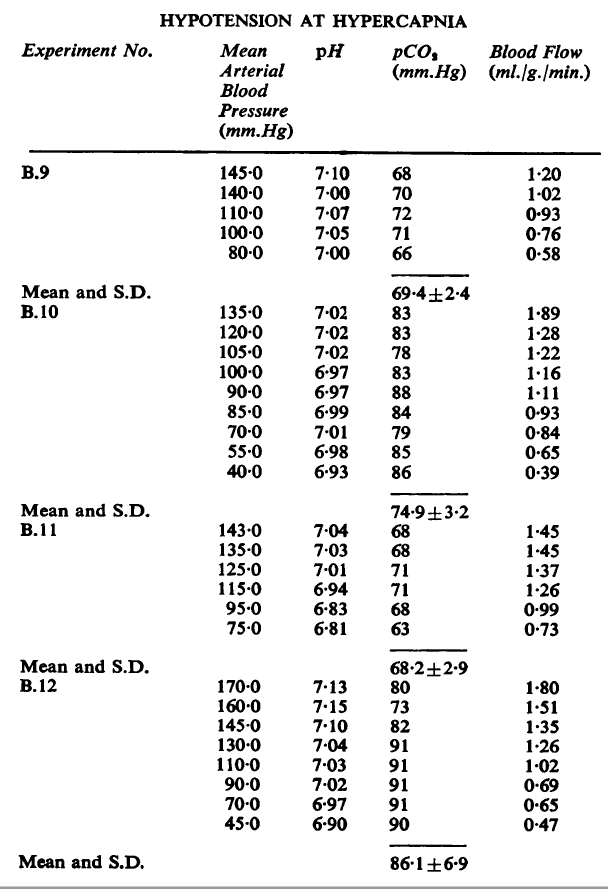
The mean values for PaCO2 for each of the four dogs in this group are 69, 83, 68, and 86 mm.Hg.
本组四只狗的 PaCO2 平均值分别为 69、83、68 和 86mm.Hg。
From Fig. 2 it can be seen that blood flow declined linearly with blood pressure.
从图 2 可以看出,血流量随着血压而线性下降。
# 讨论
It would appear that the experiments shown on Fig. 1 indicate the existence of autoregulation of blood flow in response to moderate changes in the arterial blood pressure. This is in agreement with studies by Carlyle and Grayson (1955) who used a heat clearance technique to obtain a qualitative index of the blood flow through the cerebral cortex in anaesthetized rabbits. These workers found that if the blood pressure was lowered from the control level of approximately 90 mm.Hg to approximately 45 mm.Hg, there was no change in the heat clearance and, by inference, the blood flow. More recently Rapela and Green (1964) estimated cerebral blood flow in dogs by measuring the venous outflow from the brain and found a marked autoregulatory response over the pressure range 90-50 mm.Hg.
看来,图 1 所示的实验表明,对动脉血压的适度变化,存在着血流的自动调节。这与 Carlyle 和 Grayson(1955)的研究一致,他们使用热清除技术获得了麻醉兔大脑皮层血流的定性指标。这些工作者发现,如果血压从大约 90 毫米汞柱的控制水平降低到大约 45 毫米汞柱,热清除没有变化,由此推断,血流也没有变化。最近,Rapela 和 Green(1964 年)通过测量大脑的静脉流出量来估计狗的脑血流量,发现在 90-50mm.Hg 的压力范围内有明显的自动调节反应。
However, other workers using isolated head perfusion techniques have denied the existence of auto- regulation and have claimed that the cerebral blood flow is passively dependent on the perfusion pressure (Geiger and Magnes, 1947; Sagawa and Guyton, 1961). Factors which could have masked autoregulation in these studies must be considered.
然而,其他使用孤立的头部灌注技术的工作者否认自动调节的存在,并声称脑血流被动地依赖于灌注压力(Geiger 和 Magnes,1947;Sagawa 和 Guyton,1961)。必须考虑这些研究中可能掩盖自动调节的因素。
Figure 2 shows that autoregulation is abolished by hypercapnia. Presumably the explanation for this is that vessels already maximally or nearly maximally dilated by hypercapnia are unable to dilate further in response to a lowered blood pressure. A passive pressure/flow relationship will then be observed. In the papers cited above, very extensive surgical trauma was inflicted in isolating the cerebral circulation and fairly deep anaesthesia must have been required. In neither study was the PaCO2 reported, but if it was elevated the resultant hypercapnic cerebral vasodilatation may have been sufficient to abolish or obscure autoregulation.
图 2 显示,自动调节被高碳酸血症所取消。据推测,对这一点的解释是,在高碳酸血症的作用下,已经最大限度或接近最大限度扩张的血管无法在血压降低的情况下进一步扩张。这样就可以观察到一种被动的压力 / 流量关系。在上面引用的论文中,在隔离脑循环时造成了非常广泛的手术创伤,肯定需要相当深的麻醉。在两项研究中都没有报告 PaCO2,但如果 PaCO2 升高,由此产生的高血压脑血管扩张可能足以取消或掩盖自动调节。
Rapela and Green (1964) observed autoregulation in autoperfused isolated cerebral circulations but not in artificially perfused preparations. The authors state that the absence of [autoregulatory] response in some experiments may be explained by the vulnerability of blood vessel resoonses to traumatic, surgical, or artificial perfusion procedures which appear to induce a near-maximal dilatation .
Rapela 和 Green(1964 年)在自体灌注的离体脑循环中观察到自动调节,但在人工灌注的制剂中没有。作者指出,在一些实验中没有 [自动调节] 反应,可能是由于血管对创伤、手术或人工灌注程序的反应的脆弱性,这些程序似乎会引起近乎最大的扩张。
It would appear then that, in the experimental animal, under normal physiological conditions, the calibre of the cerebral blood vessels can be adjusted to maintain a constant blood flow in the face of fairly wide fluctuations in the arterial blood pressure. However, under certain abnormal conditions, hypercapnia for instance, or probably any condition which produced an existing near-maximal dilatation, autoregulation is reduced or absent.
这样看来,在实验动物中,在正常的生理条件下,脑血管的口径可以被调整,以便在面对动脉血压相当大的波动时保持稳定的血流。然而,在某些不正常的条件下,例如高碳酸血症,或者可能是任何产生现有的接近最大扩张的条件,自动调节就会减少或没有。
MECHANISM OF AUTOREGULATION In the studies of the pial blood vessels by Fog (1938), in which vasoconstriction was demonstrated on raising the blood pressure and vasodilatation on lowering the blood pressure, the response was not affected by sectioning of the vagi, cervical sympathetic, or the sinus and aortic nerves.
自动调节的机制 在 Fog(1938 年)对皮层血管的研究中,提高血压时表现为血管收缩,降低血压时表现为血管舒张,这种反应不受切断血管、颈部交感神经或窦和主动脉神经的影响。
It appears probable, therefore, that autoregulation is effected by some local intrinsic mechanism and not by nervous control from the sympathetic or parasympathetic nervous systems.
因此,自动调节似乎很可能是由一些局部的内在机制产生的,而不是由交感或副交感神经系统的神经控制。
Lassen (1959) has suggested two possible mechanisms which could effect autoregulation of cerebral blood flow in response to changes in aterial blood pressure.
Lassen (1959) 提出了两种可能的机制,它们可以对动脉血压的变化影响脑血流的自动调节。
1 The myogenic theory Studies of segments of isolated arteries by Bayliss in 1902, suggested that alteration of intravascular pressure will produce an automatic response from the smooth muscle in the vessel wall, namely, contraction in response to a rise in pressure and relaxation in response to a drop in pressure. As this property is seen in segments of vessel perfused in vitro, it appears to be independent of nervous mechanisms.
1 肌源性理论 Bayliss 在 1902 年对离体动脉段的研究表明,血管内压力的改变会使血管壁上的平滑肌产生自动反应,即压力升高时收缩,压力下降时放松。由于这种特性在体外灌注的血管段中可以看到,它似乎与神经机制无关。
2 The metabolic theory Lassen suggested that alterations in diameter of vessels following changes in blood pressure could be mediated through alterations in the tissue and blood tensions of oxygen and carbon dioxide.
2 代谢理论 Lassen 提出,血压变化后血管直径的改变可能是通过组织和血液中氧气和二氧化碳张力的改变来介导的。
One factor which might point against the myogenic theory is the speed of response of the cerebral blood vessels to changes in blood pressure. Fog (1938) demonstrated that there was vasodilatation of the pial blood vessels following a gradual reduction in the arterial blood pressure. However, he pointed out that following a sudden reduction in blood pressure, no vasodilatation was apparent for one or two minutes. Similarly, Schneider (1963) quotes Hirsch as demonstrating in the experimental animal that a sudden decrease in systemic blood pressure from 200 to 100 mm.Hg caused a marked reduction in cerebral blood flow. More than two minutes later, however, the blood flow had almost returned to the control level. Also Rapela and Green (1964) have reported a similar marked decrease in flow following a sudden drop in blood pressure, returning to control values, however, in only 30 seconds.
一个可能反对肌源性理论的因素是脑血管对血压变化的反应速度。福格(1938 年)证明,在动脉血压逐渐降低后,皮层血管会出现血管扩张。然而,他指出,在血压突然降低后,一两分钟内没有明显的血管舒张。同样,Schneider(1963 年)引用了 Hirsch 在实验动物中的证明,全身血压从 200mm.Hg 突然下降到 100mm.Hg 会引起脑血流的明显减少。然而,两分多钟后,血流几乎恢复到了控制水平。Rapela 和 Green (1964) 也报告了在血压突然下降后,血流也有类似的明显减少,但仅在 30 秒内就恢复到控制值。
If the response of the cerebral blood vessels to a change in blood pressure was caused by a local myogenic reflex in the smooth muscle of the vessel wall, one might expect this to occur rapidly and the response would be unlikely to have a time lag of some 30 seconds to two minutes.
如果脑血管对血压变化的反应是由血管壁平滑肌的局部肌源性反射引起的,人们可能期望这种反应迅速发生,而且反应不可能有大约 30 秒到 2 分钟的时间滞后。
On the other hand, a time lag might easily occur if a metabolic factor were involved. A reasonable explanation of the phenomenon of autoregulation could be as follows. A decrease in blood pressure is followed by a reduction in blood flow. Thereafter, the tension of oxygen in the tissues will fall progressively and the tension of carbon dioxide will rise. Both the low P02 and high PCO2 will tend to cause cerebral vasodilatation with the eventual return of the blood flow to its initial value. Such a sequence of events could account for a slight time lag before the onset of autoregulation.
另一方面,如果有代谢因素的参与,则很容易出现时间滞后。对自动调节现象的合理解释可以是这样的。血压下降后,血流减少。此后,组织中氧气的张力将逐渐下降,二氧化碳的张力将上升。低 P02 和高 PCO2 都会导致脑血管扩张,最终血流恢复到初始值。这样的事件序列可以解释自律调节开始前的一个轻微的时间滞后。
Unfortunately, there is little direct evidence to support such a theory and this must await measurement of the tensions of 02 and CO2 in cerebral tissue during alterations in systemic blood pressure. However, studies by Carrier, Walker, and Guyton (1964) have shown that there is a twofold increase in conductance in isolated strips of artery (0 5-1 mm. in diameter) perfused with blood, when the P02 of the perfusate was lowered from 100 to 30 mm.Hg, this response being relatively greater in the smaller than in the larger vessels. Similarly, it has been shown by experiments in vitro that CO2 dissolved in Ringer solution dilates isolated strips of artery (Cow, 1911).
不幸的是,没有什么直接的证据来支持这样的理论,这必须等待对全身血压改变时脑组织中的 02 和 CO2 的张力进行测量。然而,Carrier、Walker 和 Guyton(1964 年)的研究表明,当灌注液的 P02 从 100 毫米汞柱降低到 30 毫米汞柱时,用血液灌注的离体动脉条(直径 0 5-1 毫米)的电导率增加了两倍,这种反应在小血管中比在大血管中相对更大。同样,体外实验表明,溶解在林格溶液中的二氧化碳可以扩张孤立的动脉条(Cow, 1911)。
If, then, one assumes that any decrease in blood flow which follows a sudden fall in pressure will result in a rise in tissue tension of CO2 and a fall in tissue tension of 02, and that this can have a local vasodilatory effect on cerebral arteries and arterioles, the metabolic theory of autoregulation becomes tenable and teleogically appropriate.
那么,如果我们假设压力突然下降后血流的任何减少都会导致二氧化碳的组织张力上升和 02 的组织张力下降,并且这可以对脑动脉和动脉血管产生局部的血管扩张作用,那么自动调节的代谢理论就变得站得住脚,并且在心灵感应上是合适的。
The absence of autoregulation in circumstances where there is pre-existing cerebral vasodilatationduring hypercapnia or hypoxia-does not negate this theory, but probably indicates that under these circumstances the vessels have reached their mechanical limit of dilatation and can respond no further to a reduction in blood pressure, resulting in a passive pressure/flow relationship.
在预先存在脑血管扩张的情况下 -- 在高碳酸血症或低氧时 -- 没有自动调节,并不能否定这一理论,但可能表明在这些情况下,血管已经达到其机械性扩张的极限,不能再对血压的降低作出反应,从而形成被动的压力 / 流量关系。
AUTOREGULATION IN MAN Extensive studies in man on the response of the cerebral blood flow to changes in blood pressure have not been carried out due to ethical considerations and methodological difficulties. However, some studies on the effect of hypertension and drug-induced hypotension have been reported in man. Lassen (1959) presented a graph of the pressure/flow relationship in man compiled from seven different sources in the literature. This study showed that neither essential nor drug-induced hypertension (Moyer, Miller, Tashnek, Snyder, and Bonman, 1953; Moyer and Morris, 1954; Hafkenschiel, Friedland, and Zintel, 1954; Moyer, Morris, Snyder, and Smith, 1954) nor hypertensive toxaemia of pregnancy caused any significant difference in blood flow when compared with results in control groups of normal young men and normal pregnant women (Kety and Schmidt, 1948; McCall, 1953). Similarly, moderate drug-induced hypotension was not associated with any significant change in blood flow (McCall, 1953).
人的自动调节 由于道德方面的考虑和方法上的困难,没有对人的脑血流对血压变化的反应进行广泛的研究。然而,一些关于高血压和药物引起的低血压影响的研究已经在人身上得到了报道。Lassen (1959) 提出了一个从文献中七个不同来源汇编的人的压力 / 流量关系图。这项研究表明,与正常青年男子和正常孕妇的对照组的结果相比,无论是基本的还是药物引起的高血压(Moyer, Miller, Tashnek, Snyder, and Bonman, 1953; Moyer and Morris, 1954; Hafkenschiel, Friedland, and Zintel, 1954; Moyer, Morris, Snyder, and Smith, 1954),还是妊娠高血压毒血症都没有造成血流量的明显差异(Kety and Schmidt, 1948; McCall, 1953)。同样,中度药物诱导的低血压也与血流的任何明显变化无关(McCall,1953)。
Lassen suggests that within a wide pressure range (approximately 60 to 170 mm.Hg) the calibre of the cerebral blood vessels can alter to compensate for changes in blood pressure. It is only in severe hypotension, that is to approximately one-third of the normal level (Finnerty, Witkin, and Fazekas, 1954), that cerebral vasodilatation is insufficient to compensate for the low arterial blood pressure, signs of cerebral ischaemia becoming apparent.
Lassen 认为,在很宽的压力范围内(约 60 至 170 毫米汞柱),脑血管的口径可以改变,以补偿血压的变化。只有在严重低血压的情况下,即达到正常水平的大约三分之一(Finnerty, Witkin, and Fazekas, 1954),脑血管扩张才不足以补偿低的动脉血压,脑缺血的迹象才会明显。
Additional studies in which measurements of cerebral blood flow were made before and after the administration of hypotensive drugs, adrenalectomy, or spinal sympathetic block, have been reported, mainly in patients with pre-existing hypertension.
还有一些研究报告,在使用降压药物、肾上腺切除术或脊髓交感神经阻断术之前和之后对脑血流进行了测量,主要是在原有高血压的病人中进行。
These can be summarized as follows:
| Series | Blood Pressure (mm.Hg) | Cerebral BloodFlow |
|---|---|---|
| Hafkenschiel et al. (1954) | Lowered from 170 to 118 | No significant change |
| Bessman, Alman, and Fazekas (1952) | Lowered from 133 to 87 | No significant change |
| Kleh and Fazekas (1956) | Lowered from 158 to 98 | No significant change |
| Moyer et al. (1953) | Lowered from 173 to 108 | No significant change |
| Stone, Mackrell, and Wechsler (1955) | Lowered from 117 to 62 | No significant change |
这些报道可归纳为以下几点。
| 序列 | 血压 (mm.Hg) | 脑血流 |
|---|---|---|
| Hafkenschiel et al. (1954) | 从 170 降至 118 | 无显著改变 |
| Bessman, Alman, and Fazekas (1952) | 从 133 降至 87 | 无显著改变 |
| Kleh and Fazekas (1956) | 从 158 降至 98 | 无显著改变 |
| Moyer et al. (1953) | 从 173 降至 108 | 无显著改变 |
| Stone, Mackrell, and Wechsler (1955) | 从 117 降至 62 | 无显著改变 |
However, contradictory findings were reported by:
| Series | Blood Pressure (mm.Hg) | Cerebral BloodFlow |
|---|---|---|
| Crumpton, Rowe, Capps, Whitmore, and Murphy (1965) | Lowered from 181 to 111 | Fall of 14% |
| Morris, Moyer, Snyder, and Haynes (1953) | Lowered from 104 to 62 | Fall of 30% |
| Kety, King, Horvath, Jeffers, and Hafkenschiel (1950) | Lowered from 155 to 106 | Fall of 12% |
然而,一些人报告了相互矛盾的发现。
| 序列 | 血压 (mm.Hg) | 脑血流 |
|---|---|---|
| Crumpton, Rowe, Capps, Whitmore, and Murphy (1965) | 从 181 降至 111 | 下降 14% |
| Morris, Moyer, Snyder, and Haynes (1953) | 从 104 降至 62 | 下降 30% |
| Kety, King, Horvath, Jeffers, and Hafkenschiel (1950) | 从 155 降至 106 | 下降 12% |
In the last study the PaCO2 fell by 5 mm.Hg, which could well account for the observed decrease in cerebral blood flow.
在最后一项研究中,PaCO2 下降了 5mm.Hg,这很可能是观察到的脑血流量减少的原因。
However, with the exception of the conflicting studies of Crumpton et al. (1955) and Morris et al. (1953), the weight of evidence seems to favour the existence of autoregulation in man. It appears that the mean arterial blood pressure can fall by at least one-third without affecting cerebral blood flow, and indeed can probably fall by more than this before affecting cerebral function and causing clinical signs of cerebral ischaemia.
然而,除了 Crumpton 等人(1955 年)和 Morris 等人(1953 年)相互矛盾的研究外,大量的证据似乎都支持人类存在自动调节功能。看来平均动脉血压至少可以下降三分之一而不影响脑血流,而且在影响脑功能和引起脑缺血的临床症状之前,确实可以下降超过这个数字。
But before one assumes that the administration of hypotensive drugs or the use of hypotensive anaesthesia will not imperil cerebral blood flow, one important point must be considered. The animal experiments reported in this paper demonstrate that, although the systemic blood pressure can be altered over a fairly wide range without affecting the cortical blood flow in normocapnic animals, there is a passive pressure/flow relationship in hypercapnic animals. Consider now a patient who has relative ischaemia of a local area of brain. Within the local ischaemic area, the blood vessels will probably be dilated under the influence of elevation of cerebral tissue PCO2 and reduction of tissue P02. This dilatation may well be sufficient to maintain a normal blood flow and the ischaemia will be 'compensated'. But if the pressure of the blood perfusing this area is now reduced, there will be a parallel reduction in blood flow (there will be no autoregulation because of pre-existing vasodilatation) with the net result of an uncompensated ischaemia. I think that this is an important point which is worthy of consideration when the administration of hypotensive drugs is contemplated.
但在人们认为服用降压药或使用降压麻醉不会危及脑血流之前,必须考虑一个重要的问题。本文所报告的动物实验表明,尽管全身血压可以在相当大的范围内改变而不影响正常血压动物的皮质血流,但在高血压动物中存在一种被动的压力 / 血流关系。现在考虑一个大脑局部区域相对缺血的病人。在局部缺血区域内,在脑组织 PCO2 升高和组织 P02 降低的影响下,血管可能会被扩张。这种扩张很可能足以维持正常的血流,缺血将得到 "补偿"。但是,如果这个区域的血液灌注压力降低,血流量也会相应减少(由于预先存在的血管扩张,不会有自动调节),最终结果是出现未补偿的缺血。我认为这是一个重要的观点,在考虑使用降压药物时值得考虑。
# 总结
Measurements of blood flow through the cerebral cortex were made in lightly anaesthetized dogs using the 85 Krypton clearance method. The systemic blood pressure was gradually reduced by bleeding. In normocapnic animals (PaCO2 30-40 mm.Hg) autoregulation of blood flow in response to changes Autoregulation ofcerebral bloodflow: influence ofbloodpressure in arterial blood pressure was observed over the range 90 to 180 mm.Hg. However, in hypercapnic animals (PaCO2 70-90 mm.Hg) where there was pre-existing cerebral vasodilatation a passive pressure/ flow relationship was observed. It was suggested that this finding may explain the failure of some previous workers to demonstrate autoregulation of cerebral blood flow in response to changes in arterial blood pressure.
在轻度麻醉的狗身上,用 85 氪清除法对通过大脑皮层的血流进行了测量。通过放血逐渐降低全身血压。在正常窒息的动物(PaCO2 30-40 mm.Hg)中,对血流变化的自律调节:在 90 至 180 mm.Hg 范围内观察到动脉血压的影响。然而,在高碳酸血症动物(PaCO2 70-90 mm.Hg)中,预先存在的脑血管舒张,观察到了被动的压力 / 流量关系。有人认为,这一发现可能解释了以前的一些工作者未能证明脑血流对动脉血压变化的自动调节。
This work was carried out in the Wellcome Surgical Research Laboratories, University of Glasgow, and supported by a grant from the Medical Research Council.
这项工作是在格拉斯哥大学的威康外科研究实验室进行的,并得到了医学研究委员会的资助。
I am grateful to Professor W. A. Mackey for his continual encouragement and advice.
我感谢 W. A. Mackey 教授的不断鼓励和建议。
# 参考文献
Bayliss, W. M. (1902). On the local reactions of the aterial wall to changes of internal pressure. J. Physiol. (Lond.), 28, 220-231.
Bayliss, W. M. (1902). 关于动脉壁对内压变化的局部反应。J. Physiol. (Lond.), 28, 220-231.
Bessman, A. N., Alman, R. W., and Fazekas, J. F. (1952). Effect of acute hypotension on cerebral hemodynamics and metabolism of elderly patients. Arch. intern. Med., 89, 893-898.
Bessman, A. N., Alman, R. W., and Fazekas, J. F. (1952). 急性低血压对老年患者的脑血流动力学和代谢的影响。Arch. intern. Med., 89, 893-898.
Carlyle, A., and Grayson, J. (1955). Blood pressure and the regulation of brain blood flow. J. Physiol., (Lond.) 127, 15P-16P.
Carlyle, A., and Grayson, J. (1955). 血压和脑血流的调节。J. Physiol., (Lond.) 127, 15P-16P.
Carrier, O., Jr., Walker, J. R., and Guyton, A. C. (1964). Role of oxygen in autoregulation of blood flow in isolated vessels. Amer. J. Physiol., 206, 951-954.
Carrier, O., Jr., Walker, J. R., and Guyton, A. C. (1964). 氧在离体血管血流自动调节中的作用。美国。J. Physiol., 206, 951-954.
Cow, D. (1911). Some reactions of surviving arteries. J. Physiol. (Lond.), 42, 125-143. (Cited by Lassen)
Cow, D. (1911). 存活动脉的一些反应。J. Physiol. (Lond.), 42, 125-143. (由 Lassen 引用)
Crumpton, C. W., Rowe, G. G., Capps, R. C., Whitmore, J. J., and Murphy, Q. R. (1955). The effect of hexamethonium upon cerebral blood flow and metabolism in patients with premalignant and malignant hypertension. Circulation, 11, 106-109.
Crumpton, C. W., Rowe, G. G., Capps, R. C., Whitmore, J. J., and Murphy, Q. R. (1955). 六甲铵对恶性高血压患者脑血流和代谢的影响。循环》,11,106-109。
Finnerty, F. A., Witkin, L., and Fazekas, J. F. (1954). Cerebral hemodynamics during cerebral ischemia induced by acute hypotension. J. clin. Invest., 33, 1227-1232.
Finnerty, F. A., Witkin, L., and Fazekas, J. F. (1954). 急性低血压引起的脑缺血期间的脑血流动力学。J. clin. Invest., 33, 1227-1232.
Fog, M. (1934). Om piaarteriernes vasomotoriske reaktioner. Munksgaard, Copenhagen. (Quoted by Lassen, N. A. (1959). Cerebral blood flow and oxygen consumption in man. Physiol. Rev., 39, 183).
Fog, M. (1934). Om piaarteriernes vasomotoriske reaktioner. Munksgaard, Copenhagen. (引自 Lassen, N. A. (1959). 人的脑血流量和耗氧量。Physiol. Rev.,39,183)。
----(1938). The relationship between the blood pressure and the tonic regulation of the pial arteries. J. Neurol. Psychiat., n.s.1, 187-197. ----(1938). 血压与皮层动脉的强直调节之间的关系。J. Neurol. Psychiat., n.s.1, 187-197. ::: ::::
Forbes, H. S., Nason, G. I., and Wortman, R. C. (1937). Cerebral circulation: vasodilation in the pia following stimulation of the vagus, aortic and carotid sinus nerves. Arch. Neurol. Psychiat. (Chic.), 37, 334-350.
Forbes, H. S., Nason, G. I., and Wortman, R. C. (1937). 脑循环:迷走神经、主动脉神经和颈动脉窦神经刺激后的皮亚血管扩张。Arch. Neurol. Psychiat. (Chic.), 37, 334-350.
Geiger, A., and Magnes, J. (1947). The isolation of the cerebral circulation and the perfusion of the brain in the living cat. Amer. J. Physiol., 149, 517-537.
Geiger, A., and Magnes, J. (1947). 活猫的脑循环和脑灌注的分离。美国。J. Physiol., 149, 517-537.
Hafkenschiel, J. H., Friedland, C. K., and Zintel, H. A. (1954). The blood flow and oxygen consumption of the brain in patients with essential hypertension before and after adrenalectomy. J. clin. Invest., 33, 57-62.
Hafkenschiel, J. H., Friedland, C. K., and Zintel, H. A. (1954). 肾上腺切除术前后原发性高血压患者的脑血流和耗氧量。J. clin. Invest., 33, 57-62.
Ingvar, D. H., and Lassen, N. A. (1962). Regional blood flow of the cerebral cortex determined by Krypton 85. Acta physiol. scand., 54, 325-338.
Ingvar, D. H., and Lassen, N. A. (1962). 由氪 85 确定的大脑皮层区域血流。Acta physiol. scand., 54, 325-338.
Kety, S. S., and Schmidt, C. F. (1948). The effects of altered arterial tensions of carbon dioxide and oxygen on cerebral blood flow and cerebral oxygen consumption of normal young men. J. clin. Invest., 27, 484-492.
Kety, S. S., and Schmidt, C. F. (1948). 二氧化碳和氧气的动脉张力改变对正常青年男子的脑血流和脑耗氧量的影响。J. clin. Invest., 27, 484-492.
----, King, B. D., Horvath, S. M., Jeffers, W. A., and Hafkenschiel, J. H. (1950). The effects of an acute reduction in blood pressure by means of differential spinal sympathetic block on the cerebral circulation of hypertensive patients. Ibid., 29,402-407. ----, King, B. D., Horvath, S. M., Jeffers, W. A., and Hafkenschiel, J. H. (1950). 通过差异性脊柱交感神经阻断对高血压患者脑循环的急性降压的影响。同上,29,402-407。 ::: ::::
Kleh, J., and Fazekas, J. F. (1956). Effects of hypotensive agents on subjects with cerebral vascular insufficiency. J. Amer. geriat. Soc., 4, 18-23.
Kleh, J., and Fazekas, J. F. (1956). 降压药对脑血管功能不全者的影响。J. Amer. geriat. Soc., 4, 18-23.
Lassen, N. A. (1959). Cerebral blood flow and oxygen consumption in man. Physiol. Rev., 39, 183-238.
Lassen, N. A. (1959). 人的脑血流量和耗氧量。Physiol. Rev., 39, 183-238.
----,and Ingvar, D. H. (1961). The blood flow of the cerebral cortex determined by radioactive Krypton. Experientia (Basel), 17, 42-43. ----,and Ingvar, D. H. (1961). 大脑皮层的血流由放射性氪确定。Experientia (Basel), 17, 42-43. ::: ::::
McCall, M. L. (1953). Cerebral circulation and metabolism in toxemia of pregnancy. Observations on the effect of Veratrum viride and Apresoline. Amer. J. Obstet. Gynec., 66, 1015-1030.
McCall, M. L. (1953). 妊娠毒血症的脑循环和新陈代谢。观察马鞭草和阿普唑仑的作用。美国。J. Obstet. Gynec., 66, 1015-1030.
Morris, G. C., Jr., Moyer, J. H., Snyder, H. B., and Haynes, B. W., Jr. (1953). Vascular dynamics in controlled hypotension. Ann. Surg., 138, 706-711.
Morris, G. C., Jr., Moyer, J. H., Snyder, H. B., and Haynes, B. W., Jr. (1953). 控制性低血压的血管动力学。Ann. Surg., 138, 706-711.
Moyer, J. H., Miller, S. I., Tashnek, A. B., Snyder, H., and Bowman, R. 0. (1953). Malignant hypertension and hypertensive encephalopathy: cerebral hemodynamic studies and therapeutic response to continuous infusion of intravenous veriloid. Amer. J. Med., 14, 175-183.
Moyer, J. H., Miller, S. I., Tashnek, A. B., Snyder, H., and Bowman, R. 0. (1953). 恶性高血压和高血压脑病:脑血流动力学研究和对静脉注射 veriloid 的治疗反应。Amer. J. Med., 14, 175-183.
----,and Morris, G. (1954). Cerebral hemodynamics during controlled hypotension induced by a continuous infusion of ganglionic blocking agents (hexamethonium, Pendiomide and Arfonad). J. clin. Invest., 33, 1081-1088. ----, 和 Morris, G. (1954). 在连续输注神经节阻断剂 (hexamethonium, Pendiomide and Arfonad) 引起的控制性低血压期间的脑血流动力学。J. clin. Invest., 33, 1081-1088. ::: ::::
----,----, Snyder, H., and Smith, C. P. (1954). A comparison of the cerebral hemodynamic response to Aramine and norepinephrine in the normotensive and hypotensive subject. Circulation, 10, 265-270. ----,----, Snyder, H., and Smith, C. P. (1954). 在正常血压和低血压患者中,对阿拉明和去甲肾上腺素的脑血流动力学反应的比较。循环》,10,265-270。 ::: ::::
Rapela, C. E., and Green, H. D. (1964). Autoregulation of canine cerebral blood flow. Circulat. Res., 15, suppl. 1, pp. 205-211.
Rapela, C. E., and Green, H. D. (1964). 犬脑血流的自动调节。循环。Res., 15, suppl. 1, pp.205-211.
Sagawa, K., and Guyton, A. C. (1961). Pressure-flow relationships in isolated canine cerebral circulation. Amer. J. Physiol., 200, 711-714.
Sagawa, K., and Guyton, A. C. (1961). 隔离的犬脑循环中的压力 - 流量关系。美国。J. Physiol., 200, 711-714.
Schneider, M. (1963). Critical blood pressure in the cerebral circulation. In Selective Vulnerability of the Brain in Hypoxaemia, edited by J. P. Schade and W. H. McMenemey. Blackwell, Oxford.
Schneider, M. (1963). 大脑循环中的临界血压。在低氧血症中大脑的选择性脆弱,由 J.P. Schade 和 W.H. McMenemey 编辑。布莱克维尔,牛津。
Sokoloff, L. (1959). The action of drugs on the cerebral circulation. Pharmacol. Rev., 11, 1-85.
Sokoloff, L. (1959). 药物对脑循环的作用。Pharmacol. Rev., 11, 1-85.
Stone, H. H., Mackrell, T. N., and Wechsler, R. L. (1955). The effect on cerebral circulation and metabolism in man of acute reduction in blood pressure by means of intravenous hexamethonium bromide and head-up tilt. Anesthesiology, 16, 168-176.
Stone, H. H., Mackrell, T. N., and Wechsler, R. L. (1955). 通过静脉注射溴化六甲铵和仰卧起坐的方式急性降低血压对人的脑循环和新陈代谢的影响。麻醉学》,16,168-176。